Abt Brittany G, Bowdish Michael E, Elsayed Ramsey S, Cohen Robbin, Bojko Markian, Vorperian Alexander, Brown Michael, Starnes Vaughn A
Division of Cardiac Surgery, Department of Surgery, University of Southern California, Keck School of Medicine, Los Angeles, Calif.
Department of Cardiac Surgery, Cedars-Sinai Medical Center, Smidt Heart Institute, Los Angeles, Calif.
JTCVS Open. 2022 Nov 16;13:106-116. doi: 10.1016/j.xjon.2022.11.004. eCollection 2023 Mar.
The study objective was to evaluate the surgical outcomes of mitral valve repair in the era of percutaneous technology.
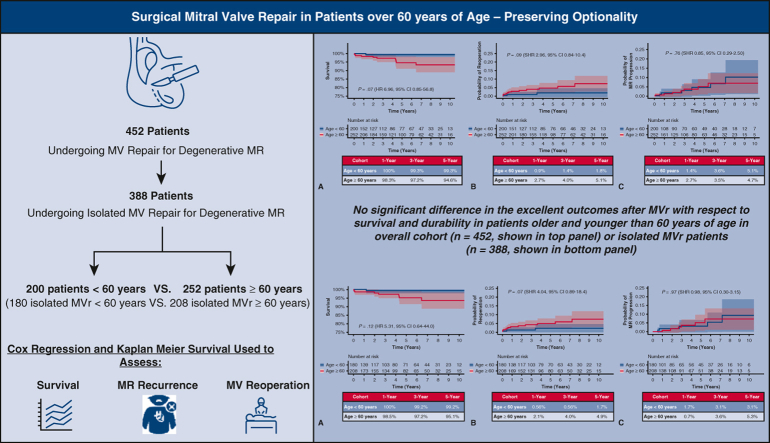
We retrospectively reviewed 452 patients who underwent mitral valve repair for degenerative disease between 2010 and 2021. Survival, mitral valve reoperation, and mitral regurgitation recurrence were assessed using Cox regression, dichotomized for those aged more than or less than 60 years.
Median age in years (interquartile range) was 52 (47-57) in the younger cohort and 67 (63-73) in the older cohort ( < .0001). Preoperative comorbidities and leaflet pathology were comparable between groups. After adjustment for sex, prior sternotomy, diabetes, atrial fibrillation, and type of leaflet repair, age 60 years or more was not associated with increased mortality (hazard ratio, 6.96, 95% confidence interval, 0.85-56.8, = .07). Considering death as a competing outcome, cumulative incidence of mitral valve reoperation at 1, 3, and 5 years was 0.9%, 1.4%, and 1.8% in the younger cohort, respectively, and 2.7%, 4.0%, and 5.1% in the older cohort, respectively (subhazard ratio, 2.95, 95% confidence interval, 0.84-10.4, = .09). Cumulative incidence of mitral regurgitation recurrence with moderate-severe or greater mitral regurgitation at 1, 3, and 5 years was 1.4%, 3.6%, and 5.1%, and 2.7%, 3.5%, and 4.7% in the younger and older cohorts, respectively (subhazard ratio, 0.85, 95% confidence interval, 0.29-2.50, = .76). Subgroup analysis focusing on isolated mitral valve repairs (n = 388) showed equivalent results with respect to mortality (hazard ratio, 5.31, 95% confidence interval, 0.64-44.0, = .12), mitral valve reoperation (subhazard ratio, 4.04, 95% confidence interval, 0.89-18.4, = .07), and mitral regurgitation recurrence (subhazard ratio, 0.98, 95% confidence interval, 0.30-3.15, = .97).
Mitral valve repair outcomes continue to be excellent, even in low-risk patients aged more than 60 years.
本研究的目的是评估经皮技术时代二尖瓣修复术的手术效果。
我们回顾性分析了2010年至2021年间因退行性疾病接受二尖瓣修复术的452例患者。使用Cox回归评估生存率、二尖瓣再次手术率和二尖瓣反流复发情况,按年龄大于或小于60岁进行二分法分析。
较年轻队列的年龄中位数(四分位间距)为52岁(47 - 57岁),较年长队列的年龄中位数(四分位间距)为67岁(63 - 73岁)(P <.0001)。两组术前合并症和瓣叶病理情况相当。在调整性别、既往胸骨切开术、糖尿病、心房颤动和瓣叶修复类型后,60岁及以上年龄与死亡率增加无关(风险比,6.96,95%置信区间,0.85 - 56.8,P =.07)。将死亡视为竞争结局,较年轻队列1年、3年和5年二尖瓣再次手术的累积发生率分别为0.9%、1.4%和1.8%,较年长队列分别为2.7%、4.0%和5.1%(亚风险比,2.95,95%置信区间,0.84 - 10.4,P =.09)。较年轻和较年长队列中,1年、3年和5年中度至重度或更严重二尖瓣反流的二尖瓣反流复发累积发生率分别为1.4%、3.6%和5.1%,以及2.7%、3.5%和4.7%(亚风险比,0.85,95%置信区间,0.29 - 2.50,P =.76)。聚焦于单纯二尖瓣修复术(n = 388)的亚组分析在死亡率(风险比,5.31,95%置信区间,0.64 - 44.0,P =.12)、二尖瓣再次手术(亚风险比,4.04,95%置信区间,0.89 - 18.4,P =.07)和二尖瓣反流复发(亚风险比,0.98,95%置信区间,0.30 - 3.15,P =.97)方面显示出相似结果。
即使在60岁以上的低风险患者中,二尖瓣修复术的效果仍然极佳。