Ding Yipu, Liu Zinuan, Wang Xi, Xin Ran, Shan Dongkai, He Bai, Jing Jing, Gao Qi, Yang Junjie, Chen Yundai
Senior Department of Cardiology, the Sixth Medical Centre, Chinese PLA General Hospital, Beijing, China.
School of Medicine, Nankai University, Tianjin, China.
Quant Imaging Med Surg. 2023 Apr 1;13(4):2339-2351. doi: 10.21037/qims-22-832. Epub 2023 Feb 9.
Development in computational fluid dynamics and 3D construction could facilitate the calculation of hemodynamic stresses in coronary computed tomography angiography (CCTA). However, the agreement between CCTA derived stresses and intravascular ultrasound/intravascular coronary angiography (IVUS/ICA)-derived stresses remains undetermined. Thus, the purpose of this study is to investigate if CCTA can serve as alternative to IVUS/ICA for hemodynamic evaluation.
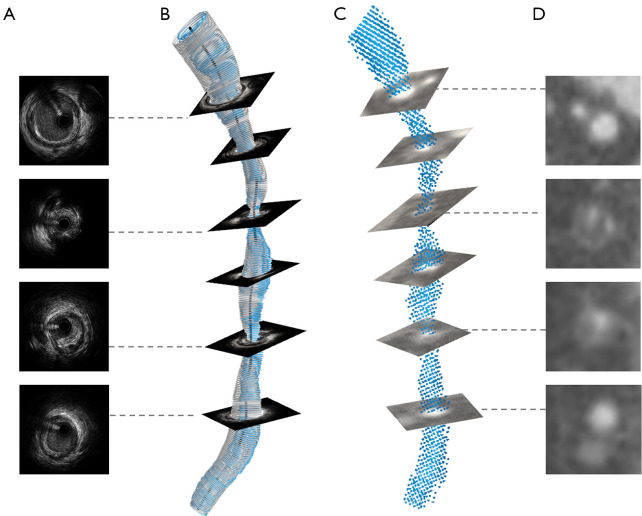
In this retrospective study, 13 patients (14 arteries) with unstable angina who underwent both CCTA and IVUS/ICA at an interval of less than 7 days were consecutively included at the Chinese PLA General Hospital within the year of 2021. Slice-level minimal lumen area (MLA), percent area stenosis, velocity, pressure, Reynolds number, wall shear stress (WSS) and axial plaque stress (APS) were determined by both modalities. The agreement between CCTA and IVUS/ICA was assessed using the intraclass correlation coefficient (ICC), Pearson's correlation coefficient and Bland-Altman analysis.
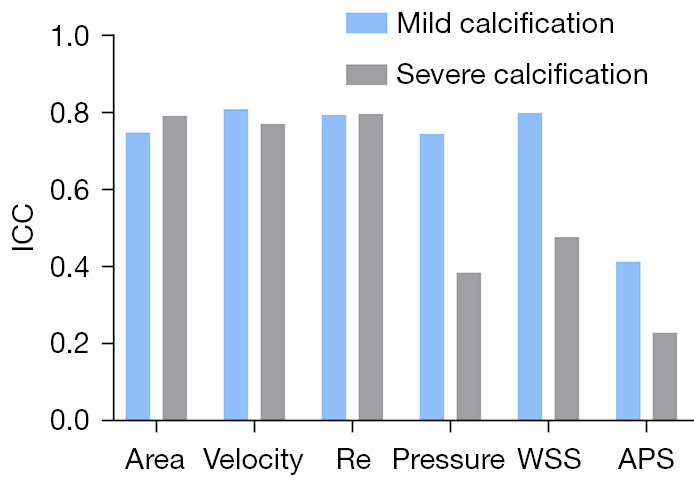
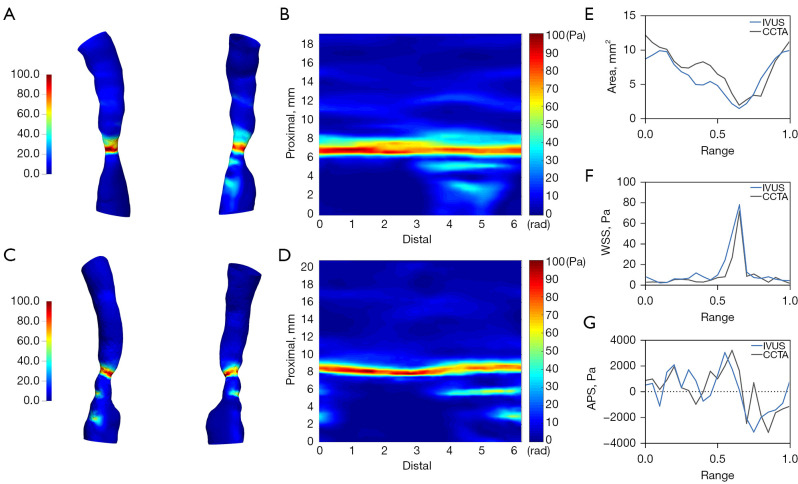
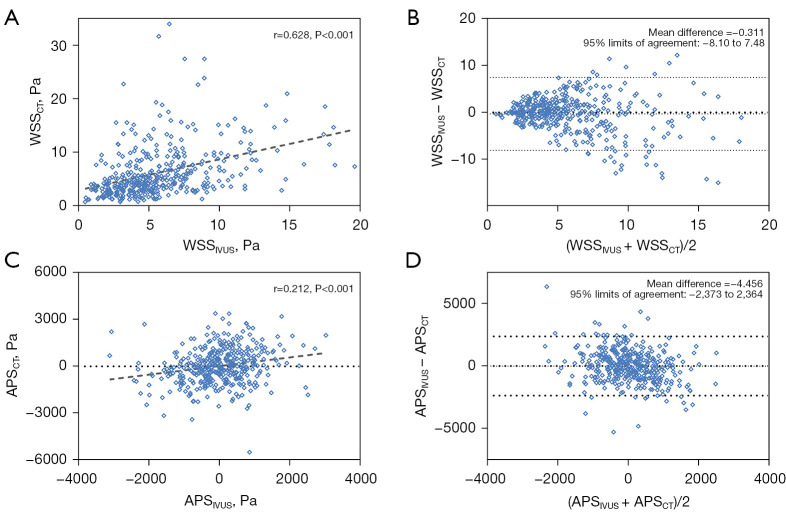
CCTA overestimated the degree of area stenosis (50.22%±16.15% . 36.41%±19.37%, P=0.004) with the MLA showing no significant difference (5.81±2.24 . 6.72±2.04 mm, P=0.126). No statistical difference was observed in WSS (6.57±6.26 . 5.98±5.55 Pa, P=0.420) and APS (16.03±1,159.45 . -1.27±890.39 Pa, P=0.691) between CCTA and IVUS. Good correlation was found in velocity (ICC: 0.796, 95% CI: 0.752-0.833), Reynolds number (ICC: 0.810, 95% CI: 0.768-0.844) and WSS (ICC: 0.769, 95% CI: 0.718-0.810), while the ICC of APS was (ICC: 0.341, 95% CI: 0.197-0.458), indicating a relatively poor correlation.
CCTA can serve as a satisfactory alternative to the reference standard, IVUS/ICA in morphology simulation and hemodynamic stress calculation, especially in the calculation of WSS.
计算流体动力学和三维建模技术的发展有助于在冠状动脉计算机断层扫描血管造影(CCTA)中计算血流动力学应力。然而,CCTA得出的应力与血管内超声/血管内冠状动脉造影(IVUS/ICA)得出的应力之间的一致性仍未确定。因此,本研究的目的是探讨CCTA能否作为IVUS/ICA的替代方法用于血流动力学评估。
在这项回顾性研究中,2021年在中国人民解放军总医院连续纳入了13例(14条动脉)患有不稳定型心绞痛且在间隔不到7天的时间内先后接受了CCTA和IVUS/ICA检查的患者。通过两种检查方式确定切片水平的最小管腔面积(MLA)、面积狭窄百分比、速度、压力、雷诺数、壁面切应力(WSS)和轴向斑块应力(APS)。使用组内相关系数(ICC)、Pearson相关系数和Bland-Altman分析评估CCTA与IVUS/ICA之间的一致性。
CCTA高估了面积狭窄程度(50.22%±16.15% 对 36.41%±19.37%,P = 0.004),而MLA无显著差异(5.81±2.24 对 6.72±2.04 mm,P = 0.126)。CCTA与IVUS之间在WSS(6.57±6.26 对 5.98±5.55 Pa,P = 0.420)和APS(16.03±1,159.45 对 -1.27±890.39 Pa,P = 0.691)方面未观察到统计学差异。在速度(ICC:0.796,95%CI:0.752 - 0.833)、雷诺数(ICC:0.810,95%CI:0.768 - 0.844)和WSS(ICC:0.769,95%CI:0.718 - 0.810)方面发现有良好的相关性,而APS的ICC为(ICC:0.341,95%CI:0.197 - 0.458),表明相关性相对较差。
在形态学模拟和血流动力学应力计算方面,尤其是在WSS计算中,CCTA可以作为参考标准IVUS/ICA的一种令人满意的替代方法。