Vuong Anh Dinh Bao, Pham Thanh Hai, Nguyen Xuan Trang, Trinh Ngoc Bich, Nguyen Phuc Nhon, Ho Quang Nhat
Department of High-Risk Pregnancy, Tu Du Hospital, Ho Chi Minh City, Vietnam.
Tu Du Clinical Research Unit (TD-CRU), Ho Chi Minh City, Vietnam.
Int J Emerg Med. 2023 Apr 17;16(1):26. doi: 10.1186/s12245-023-00498-w.
Spontaneous hemoperitoneum in pregnancy (SHiP) refers to fluid collection in the abdominal cavity with a vague presentation of clinical symptoms. Particularly, SHiP causes a life-threatening condition with the coexistence of intrauterine pregnancy, since this dangerous complication significantly increases the maternal and fetal mortality. Herein, we present two cases of nontraumatic SHiP in the second and third trimester of pregnancy, respectively.
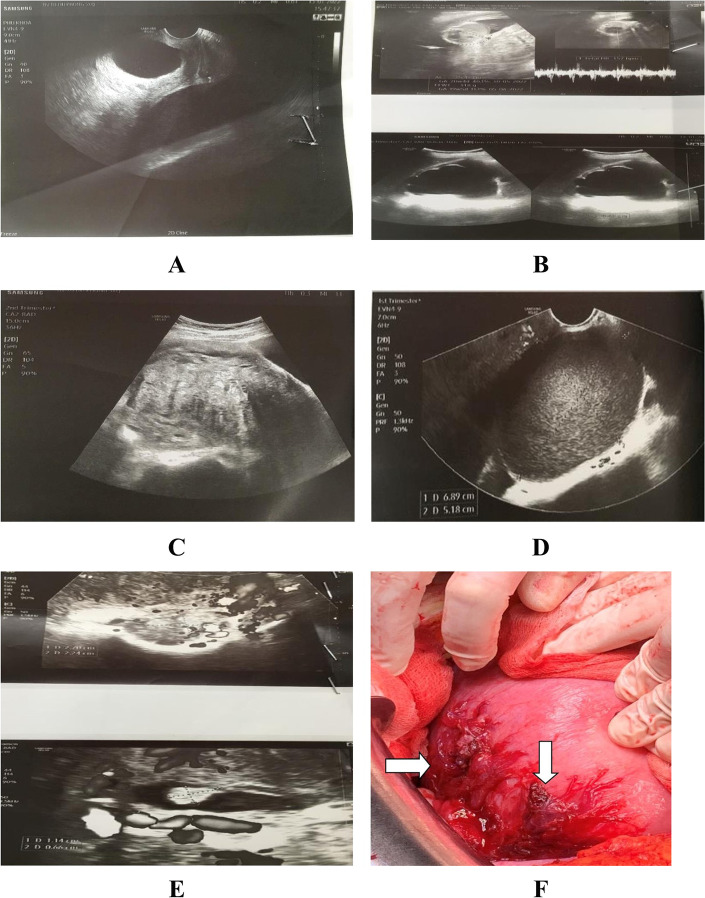
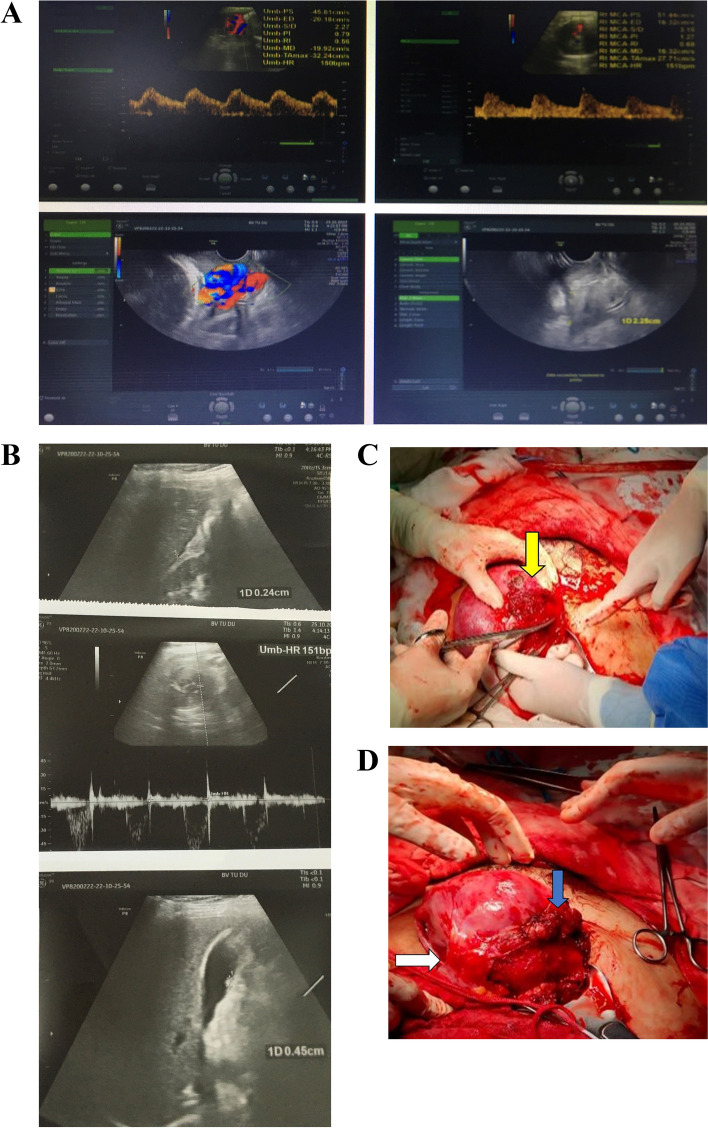
The pregnant woman in case 1 was admitted to our hospital owing to severe paroxysmal shoulder pain along with abdominal pain. Her medical history was remarkably recorded with endometriosis and adenomyosis. At the emergency room, an ultrasound scan revealed a live fetus corresponding to 21 weeks and 3 days and free fluid in the abdominal cavity. She was subsequently diagnosed with SHiP and underwent immediate laparotomy for hemostatic procedures. During the postpartum course, the patient was uneventfully monitored. Unfortunately, the patient delivered on the 4th postoperative day in spite of the initial administration of tocolytic agents and close monitoring. The primigravid woman in case 2 complained of lower abdominal pain and vaginal bleeding. The patient's history was noted with ovarian tumor removal. At admission, the sonography scan revealed free fluid in the abdominal cavity, a fetus at 34 weeks and 3 days gestational age with bradycardia of 70 bpm, and a laboratory test showed a low hemoglobin level. Thus, exploratory laparotomy and hysterotomy were performed at the same time due to fetal distress. The postpartum course was uneventful. The patient was discharged 5 days later.
In pregnant women with a history of endometriosis, adenomyosis, or ovarian tumor removal, acute abdominal pain combined with the presence of free fluid collection in the intraperitoneal cavity, and a decreased hemoglobin levels should be first assessed as SHiP originating from the spontaneous rupture of abnormal vascular proliferation. Proper management is strongly indicated for an emergent laparotomy to control the active bleeding point, thus increasing the survival rate for both mother and neonate.
妊娠期自发性腹腔内出血(SHiP)是指腹腔内积液,临床症状表现模糊。特别是,SHiP会因合并宫内妊娠而导致危及生命的情况,因为这种危险的并发症会显著增加母婴死亡率。在此,我们分别介绍两例妊娠中晚期非创伤性SHiP病例。
病例1中的孕妇因严重阵发性肩痛伴腹痛入院。其病史显著记录有子宫内膜异位症和子宫腺肌病。在急诊室,超声扫描显示有一个相当于21周零3天的活胎以及腹腔内游离液体。她随后被诊断为SHiP,并立即接受剖腹手术进行止血操作。在产后过程中,对患者进行了平稳监测。不幸的是,尽管最初使用了宫缩抑制剂并进行了密切监测,但患者在术后第4天分娩。病例2中的初产妇主诉下腹痛和阴道出血。该患者有卵巢肿瘤切除病史。入院时,超声检查显示腹腔内有游离液体,一个孕34周零3天的胎儿心率为70次/分,心动过缓,实验室检查显示血红蛋白水平低。因此,由于胎儿窘迫,同时进行了剖腹探查术和子宫切开术。产后过程平稳。患者5天后出院。
对于有子宫内膜异位症、子宫腺肌病或卵巢肿瘤切除病史的孕妇,急性腹痛合并腹腔内有游离液体以及血红蛋白水平降低,应首先评估为源于异常血管增生自发破裂的SHiP。强烈建议进行适当管理,紧急进行剖腹手术以控制活跃出血点,从而提高母亲和新生儿的存活率。