Costa Maria Adriano, Pimentel Alice, da Silva Sofia Dias, Sardo Leonor, Moreira Rui, Noronha Joana
General Surgery Department, Centro Hospitalar do Baixo Vouga, Aveiro, Portugal.
Int J Surg Case Rep. 2023 May;106:108170. doi: 10.1016/j.ijscr.2023.108170. Epub 2023 Apr 11.
Spontaneous perforation of the biliary tree, resulting in retroperitoneal biloma in adults is an extremely rare condition, and may unfold to a potentially fatal outcome, particularly when the diagnosis and definitive treatment are delayed.
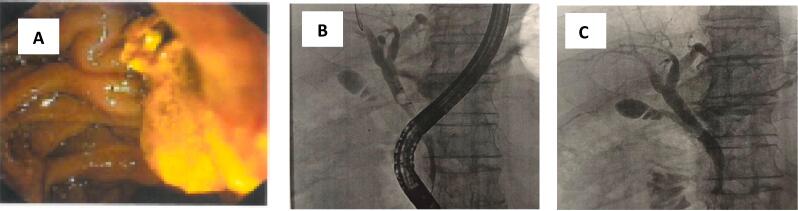
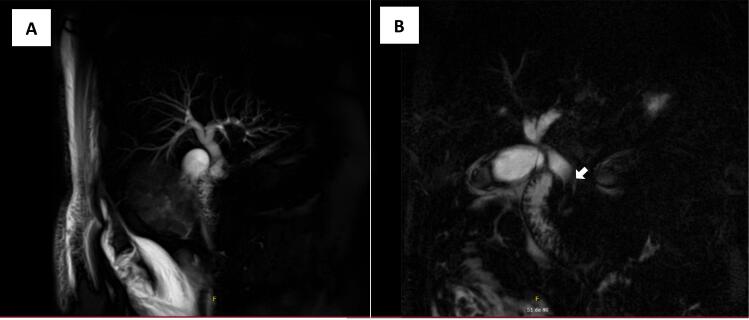
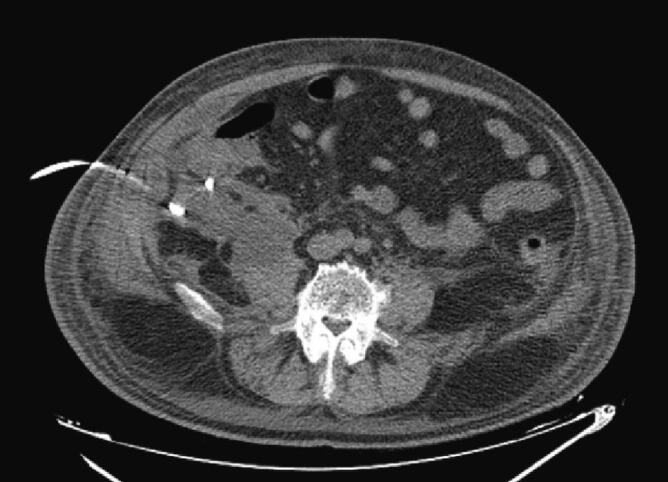
We report a case of a 69-year-old male who presented to the emergency room with abdominal pain, localized to the right quadrants, associated with jaundice and dark-coloured urine. Abdominal imaging including CT scan, ultrasound and magnetic resonance cholangiopancreatography (MRCP) revealed a retroperitoneal fluid collection, a distended gallbladder with wall thickening and lithiasis, as well as a dilated common bile duct (CBD) with choledocholithiasis. The analysis of the retroperitoneal fluid obtained by CT-guided percutaneous drainage was consistent with biloma. A combined approach of biloma percutaneous drainage and endoscopic retrograde cholangiopancreatography (ERCP)-guided stent placement in the CBD with biliary stones removal was successful in the management of this patient, despite the fact that the perforation site could not be detected.
The diagnosis of biloma is based mainly on clinical presentation and abdominal imaging. If urgent surgical intervention is not indicated, pressure necrosis and perforation of the biliary tree may be avoided by timely percutaneous aspiration of the biloma and ERCP to remove the impacted stones in the biliary tree.
Biloma should be considered in the differential diagnosis of a patient presenting with right upper quadrant or epigastric pain and an intra-abdominal collection on imaging. Efforts should be made in order to offer a prompt diagnosis and treatment to the patient.
成人胆管自发性穿孔导致腹膜后胆汁瘤是一种极为罕见的病症,可能会发展为潜在的致命后果,尤其是在诊断和确定性治疗延迟的情况下。
我们报告一例69岁男性患者,因腹痛就诊于急诊室,腹痛局限于右腹象限,伴有黄疸和深色尿液。包括CT扫描、超声和磁共振胰胆管造影(MRCP)在内的腹部影像学检查显示腹膜后有液体积聚、胆囊扩张伴壁增厚和结石形成,以及胆总管(CBD)扩张伴胆总管结石。经CT引导下经皮穿刺引流获得的腹膜后液体分析结果与胆汁瘤一致。尽管未能检测到穿孔部位,但采用胆汁瘤经皮穿刺引流联合内镜逆行胰胆管造影(ERCP)引导下在CBD放置支架并取出胆管结石的联合方法成功治疗了该患者。
胆汁瘤的诊断主要基于临床表现和腹部影像学检查。如果不建议进行紧急手术干预,通过及时经皮抽吸胆汁瘤和ERCP以清除胆管内嵌顿结石,可避免胆管的压力性坏死和穿孔。
对于出现右上腹或上腹部疼痛且影像学检查发现腹腔内有液体积聚的患者,鉴别诊断时应考虑胆汁瘤。应努力为患者提供及时的诊断和治疗。