Feliciano Josephine Louella, McLoone Dylan, Xu Yingxin, Quek Ruben G W, Kuznik Andreas, Pouliot Jean-Francois, Gullo Giuseppe, Rietschel Petra, Guyot Patricia, Konidaris Gerasimos, Chan Keith, Keeping Sam, Wilson Florence R, Freemantle Nick
Johns Hopkins University, Baltimore, MD, United States.
PRECISIONheor, Boston, MA, United States.
Front Oncol. 2023 Apr 4;12:1081729. doi: 10.3389/fonc.2022.1081729. eCollection 2022.
In randomized-controlled crossover design trials, overall survival (OS) treatment effect estimates are often confounded by the control group benefiting from treatment received post-progression. We estimated the adjusted OS treatment effect in EMPOWER-Lung 1 (NCT03088540) by accounting for the potential impact of crossover to cemiplimab among controls and continued cemiplimab treatment post-progression.
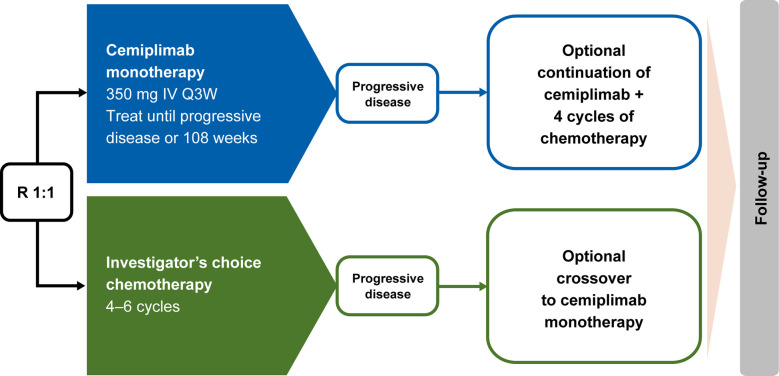
Patients were randomly assigned 1:1 to cemiplimab 350 mg every 3 weeks (Q3W) or platinum-doublet chemotherapy. Patients with disease progression while on or after chemotherapy could receive cemiplimab 350 mg Q3W for ≤108 weeks. Those who experienced progression on cemiplimab could continue cemiplimab at 350 mg Q3W for ≤108 additional weeks with four chemotherapy cycles added. Three adjustment methods accounted for crossover and/or continued treatment: simplified two-stage correction (with or without recensoring), inverse probability of censoring weighting (IPCW), and rank-preserving structural failure time model (RPSFT; with or without recensoring).
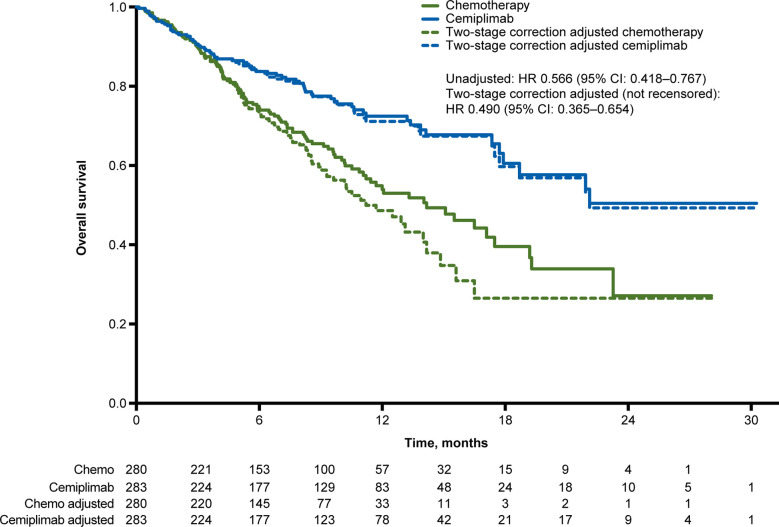
In the programmed cell death-ligand 1 ≥50% population (N=563; median 10.8-month follow-up), 38.2% (n=107/280) crossed over from chemotherapy to cemiplimab (71.3%, n=107/150, among those with confirmed progression) and 16.3% (n=46/283) received cemiplimab treatment after progression with the addition of histology-specific chemotherapy (38.7%, n=46/119, among those with confirmed progression). The unadjusted OS hazard ratio (HR) with cemiplimab versus chemotherapy was 0.566 (95% confidence interval [CI]: 0.418, 0.767). Simplified two-stage correction-the most suitable method based on published guidelines and trial characteristics-produced an OS HR of 0.490 (95% CI: 0.365, 0.654) without recensoring and 0.493 (95% CI: 0.361, 0.674) with recensoring. The IPCW and RPSFT methods produced estimates generally consistent with simplified two-stage correction.
After adjusting for treatment crossover and continued cemiplimab treatment after progression with the addition of histology-specific chemotherapy observed in EMPOWER-Lung 1, cemiplimab continued to demonstrate a clinically important and statistically significant OS benefit versus chemotherapy, consistent with the primary analysis.
在随机对照交叉设计试验中,总生存期(OS)治疗效果估计值常常因对照组在病情进展后接受治疗而受益受到混淆。我们通过考虑对照组交叉接受西米普利单抗以及病情进展后继续接受西米普利单抗治疗的潜在影响,对EMPOWER-Lung 1(NCT03088540)试验中经调整的OS治疗效果进行了估计。
患者按1:1随机分配,每3周接受一次350mg西米普利单抗(Q3W)或铂类双联化疗。化疗期间或化疗后病情进展的患者可接受每3周一次350mg西米普利单抗治疗,持续≤108周。接受西米普利单抗治疗后病情进展的患者可继续每3周一次350mg西米普利单抗治疗,持续≤108周,并增加四个化疗周期。三种调整方法考虑了交叉和/或继续治疗的情况:简化两阶段校正(有或无重新删失)、删失逆概率加权法(IPCW)和秩保持结构失效时间模型(RPSFT;有或无重新删失)。
在程序性死亡配体1≥50%的人群中(N = 563;中位随访10.8个月),3(n = 107/280)从化疗交叉接受西米普利单抗治疗(在确诊病情进展的患者中为71.3%,n = 107/150),16.3%(n = 46/283)在病情进展后接受西米普利单抗治疗并增加了组织学特异性化疗(在确诊病情进展的患者中为38.7%,n = 46/119)。西米普利单抗与化疗相比,未经调整的OS风险比(HR)为0.566(95%置信区间[CI]:0.418,0.767)。简化两阶段校正——基于已发表的指南和试验特征最适合的方法——在无重新删失时得出OS HR为0.490(95%CI:0.365,0.654),在有重新删失时为0.493(95%CI:0.361,0.674)。IPCW和RPSFT方法得出的估计值与简化两阶段校正总体一致。
在对EMPOWER-Lung 1试验中观察到的治疗交叉以及病情进展后继续接受西米普利单抗治疗并增加组织学特异性化疗进行调整后,与化疗相比,西米普利单抗继续显示出具有临床重要意义且在统计学上显著的OS获益,与初步分析结果一致。