Nilsen Per, Ingvarsson Sara, Hasson Henna, von Thiele Schwarz Ulrica, Augustsson Hanna
Division of Public Health, Department of Health, Medical and Caring Sciences, Linköping University, Linköping, Sweden.
Procome Research Group, Medical Management Centre, Karolinska Institutet, Stockholm, Sweden.
Implement Res Pract. 2020 Sep 18;1:2633489520953762. doi: 10.1177/2633489520953762. eCollection 2020 Jan-Dec.
The aim of this scoping review was to identify theories, models, and frameworks for understanding the processes and determinants of de-implementing low-value care (LVC). We investigated theories, models, and frameworks developed specifically for de-implementation of LVC (conceptual studies) and those that were originally developed for implementation of evidence-based practices but were applied in studies to analyze de-implementation of LVC (empirical studies).
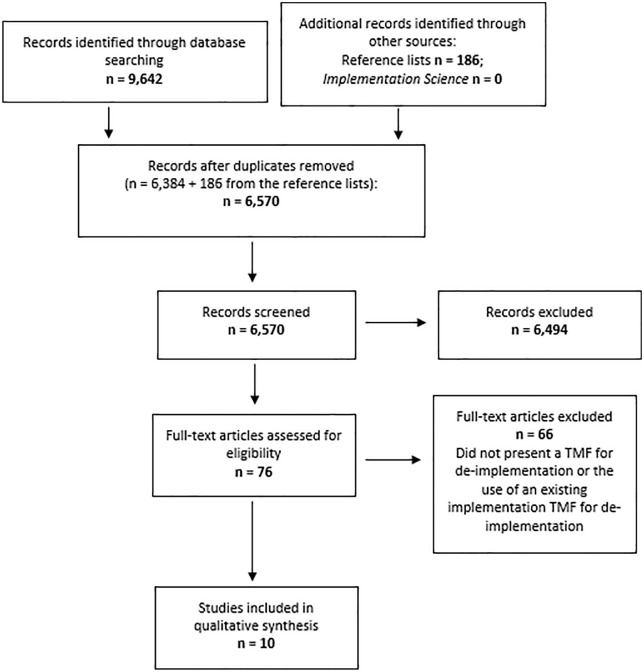
We performed a scoping review to identify theories, models, and frameworks used to describe, guide, or explain de-implementation of LVC, encompassing four stages following the identification of the research question: (1) identifying relevant studies; (2) study selection; (3) charting the data; and (4) collating, summarizing, and reporting the results. The database searches yielded 9,642 citations. After removing duplicates, 6,653 remained for the abstract screening process. After screening the abstracts, 76 citations remained. Of these, 10 studies were included in the review.
We identified 10 studies describing theories, models, and frameworks that have been used to understand de-implementation of LVC. Five studies presented theories, models, or frameworks developed specifically for de-implementation of LVC (i.e., conceptual studies) and five studies applied an existing theory, model, or framework concerning implementation of evidence-based practices (i.e., empirical studies).
Most of the theories, models, and frameworks that are used to analyze LVC suggest a multi-level understanding of de-implementation of LVC. The role of the patient is inconsistent in these theories, models, and frameworks; patients are accounted for in some but not in others. The findings point to the need for more research to identify the most important processes and determinants for successful de-implementation of LVC and to explore differences between de-implementation and implementation.
Achieving an evidence-based practice not only depends on implementation of evidence-based interventions (programs, methods, etc.) but also requires de-implementing interventions that are evidence-based, that is, low-value care (LVC). Thus, de-implementation is the other side of the coin of an evidence-based practice. However, this is quite a new topic and knowledge is lacking concerning how de-implementation and implementation processes and determinants might differ. It is almost mandatory for implementation researchers to use theories, models, and frameworks (i.e., "theoretical approaches") to describe, guide, or explain implementation processes and determinants. To what extent are such approaches also used with regard to de-implementation of LVC? And what are the characteristics of such approaches when analyzing de-implementation processes? We reviewed the literature to explore issues such as these. We identified only 10 studies describing theoretical approaches that have been used concerning de-implementation of LVC. Five studies presented approaches developed specifically for de-implementation of LVC and five studies applied an already-existing approach usually applied to analyze implementation processes. Most of the theoretical approaches we found suggest a multi-level understanding of de-implementation of LVC, that is, successfully de-implementing LVC may require strategies that target teams, departments, and organizations and merely focus on individual health care practitioners. The findings point to the need for more research to identify the most important processes and determinants for successful de-implementation of LVC, and to explore differences between de-implementation and implementation. In terms of practice and policy implications, the study underscores the relevance of addressing multiple levels when attempting to de-implement LVC.
本范围综述的目的是确定用于理解低价值医疗(LVC)去实施过程和决定因素的理论、模型和框架。我们调查了专门为LVC去实施而开发的理论、模型和框架(概念性研究),以及最初为循证实践实施而开发但在研究中用于分析LVC去实施的理论、模型和框架(实证研究)。
我们进行了一项范围综述,以确定用于描述、指导或解释LVC去实施的理论、模型和框架,包括确定研究问题后的四个阶段:(1)识别相关研究;(2)研究选择;(3)梳理数据;(4)整理、总结和报告结果。数据库检索产生了9642条引文。去除重复项后,6653条剩余用于摘要筛选过程。筛选摘要后,剩余76条引文。其中,10项研究被纳入综述。
我们确定了10项描述用于理解LVC去实施的理论、模型和框架的研究。5项研究提出了专门为LVC去实施而开发的理论、模型或框架(即概念性研究),5项研究应用了关于循证实践实施的现有理论、模型或框架(即实证研究)。
大多数用于分析LVC的理论、模型和框架表明对LVC去实施有多层次的理解。患者在这些理论、模型和框架中的作用不一致;有些考虑了患者,有些则没有。研究结果表明需要更多研究来确定成功去实施LVC的最重要过程和决定因素,并探索去实施与实施之间的差异。
实现循证实践不仅取决于循证干预措施(项目、方法等)的实施,还需要去除那些没有循证依据的干预措施,即低价值医疗(LVC)。因此,去实施是循证实践的另一面。然而,这是一个相当新的话题,关于去实施过程和决定因素与实施过程和决定因素可能存在的差异,我们还缺乏相关知识。实施研究人员几乎必须使用理论、模型和框架(即“理论方法”)来描述、指导或解释实施过程和决定因素。在LVC去实施方面,这些方法在多大程度上也被使用?分析去实施过程时这些方法有哪些特点?我们回顾了文献以探讨诸如此类的问题。我们仅确定了10项描述用于LVC去实施的理论方法的研究。5项研究提出了专门为LVC去实施而开发的方法,5项研究应用了通常用于分析实施过程的现有方法。我们发现的大多数理论方法表明对LVC去实施有多层次的理解,也就是说,成功去实施LVC可能需要针对团队、部门和组织的策略,而不仅仅关注个体医疗保健从业者。研究结果表明需要更多研究来确定成功去实施LVC的最重要过程和决定因素,并探索去实施与实施之间的差异。在实践和政策影响方面,该研究强调了在尝试去实施LVC时应对多个层面问题的相关性。