Oishi Keiji, Hamada Kazuki, Murata Yoriyuki, Matsuda Kazuki, Ohata Syuichiro, Yamaji Yoshikazu, Asami-Noyama Maki, Edakuni Nobutaka, Kakugawa Tomoyuki, Hirano Tsunahiko, Matsunaga Kazuto
Department of Respiratory Medicine and Infectious Disease, Graduate School of Medicine, Yamaguchi University, Ube 755-8505, Japan.
Department of Pulmonology and Gerontology, Graduate School of Medicine, Yamaguchi University, Ube 755-8505, Japan.
J Clin Med. 2023 Apr 16;12(8):2900. doi: 10.3390/jcm12082900.
Recent advances in biologics have provided new insights into the clinical course of asthma, including disease modification, clinical remission (CR), and deep remission (DR). However, the extent to which biologics achieve CR and DR in severe asthma patients is poorly understood.
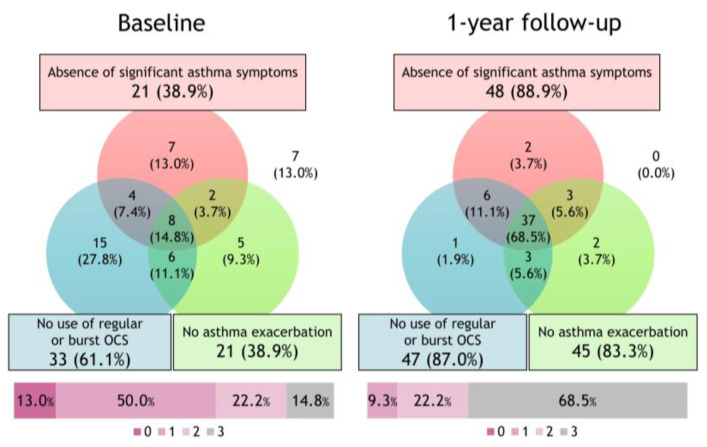
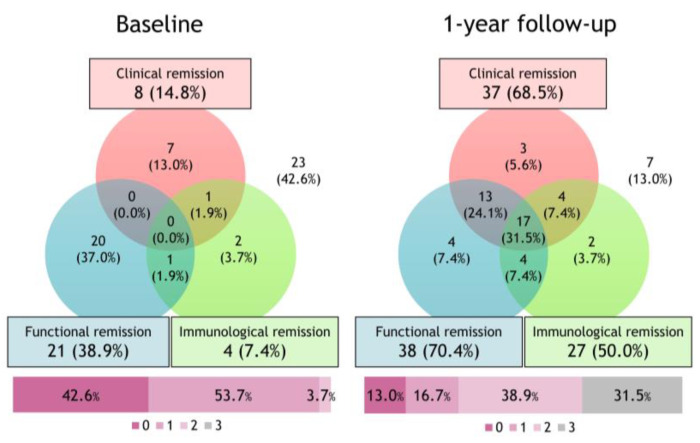
To assess the achievement rate and predictors of CR and DR using long-term biologics, we retrospectively evaluated 54 severe asthma patients recently started on biologics. "CR" denotes the achievement of all three criteria: (1) absence of asthma symptoms, (2) no asthma exacerbations, and (3) no use of oral corticosteroids. DR denoted CR plus (4) normalized pulmonary function and (5) suppressed type 2 inflammation.
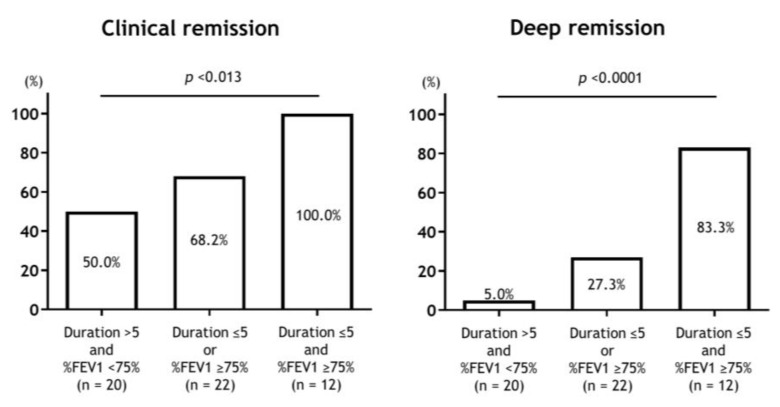
CR and DR achievement rates were 68.5% and 31.5%, respectively. Compared with the non-deep remission group, the DR group had higher adult-onset asthma rates (94.1% vs. 70.3%, = 0.078), shorter asthma duration (5 vs. 19 years, = 0.006), and higher FEV (91.5% vs. 71.5%, < 0.001). There were no significant differences in the Asthma Control Questionnaire scores, exacerbation frequency, or type 2 inflammation at baseline between groups. Asthma duration combined with FEV can stratify the achievement rates of CR and DR.
the early introduction of biologics in severe asthma patients may help achieve CR and DR.
生物制剂的最新进展为哮喘的临床病程提供了新的见解,包括疾病改善、临床缓解(CR)和深度缓解(DR)。然而,生物制剂在重度哮喘患者中实现CR和DR的程度尚不清楚。
为了评估使用长效生物制剂实现CR和DR的成功率及预测因素,我们回顾性评估了54例近期开始使用生物制剂的重度哮喘患者。“CR”表示达到以下所有三个标准:(1)无哮喘症状,(2)无哮喘加重,(3)未使用口服糖皮质激素。DR表示CR加上(4)肺功能正常化和(5)2型炎症受到抑制。
CR和DR的实现率分别为68.5%和31.5%。与非深度缓解组相比,DR组成人起病哮喘的发生率更高(94.1%对70.3%,P = 0.078),哮喘病程更短(5年对19年,P = 0.006),FEV更高(91.5%对71.5%,P < 0.001)。两组之间在基线时的哮喘控制问卷评分、加重频率或2型炎症方面无显著差异。哮喘病程与FEV相结合可以对CR和DR的实现率进行分层。
在重度哮喘患者中早期引入生物制剂可能有助于实现CR和DR。