Veerman G D Marijn, Boosman Rene J, Jebbink Merel, Oomen-de Hoop Esther, van der Wekken Anthonie J, Bahce Idris, Hendriks Lizza E L, Croes Sander, Steendam Christi M J, de Jonge Evert, Koolen Stijn L W, Steeghs Neeltje, van Schaik Ron H N, Smit Egbert F, Dingemans Anne-Marie C, Huitema Alwin D R, Mathijssen Ron H J
Department of Medical Oncology, Erasmus MC Cancer Institute, Erasmus University Medical Centre, Rotterdam, the Netherlands.
Department of Pulmonary Medicine, Erasmus MC Cancer Institute, Erasmus University Medical Center, Rotterdam, the Netherlands.
EClinicalMedicine. 2023 Apr 13;59:101955. doi: 10.1016/j.eclinm.2023.101955. eCollection 2023 May.
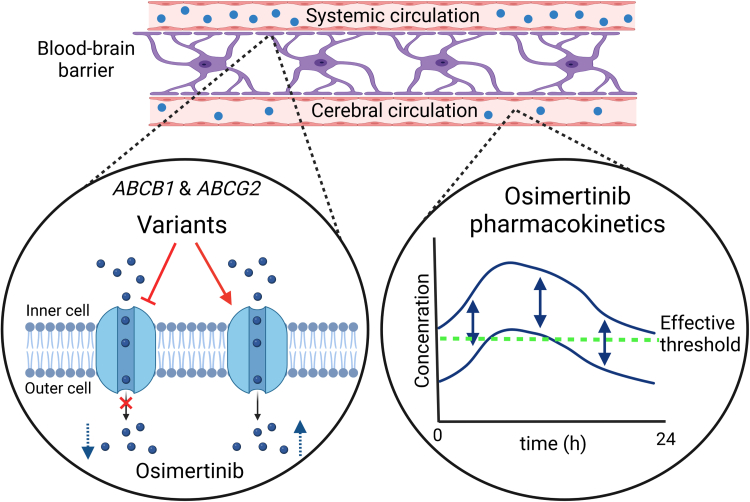
Central nervous system (CNS) metastases are present in approximately 40% of patients with metastatic epidermal growth factor receptor-mutated (m+) non-small cell lung cancer (NSCLC). The EGFR-tyrosine kinase inhibitor osimertinib is a substrate of transporters ABCB1 and ABCG2 and metabolized by CYP3A4. We investigated relationships between single nucleotide polymorphisms (SNPs) 3435C>T, 421C>A and 34G>A, and and CNS treatment efficacy of osimertinib in m+ NSCLC patients.
Patients who started treatment with osimertinib for m+ NSCLC between November 2014 and June 2021 were included in this retrospective observational multicentre cohort study. For patients with baseline CNS metastases, the primary endpoint was CNS progression-free survival (CNS-PFS; time from osimertinib start until CNS disease progression or death). For patients with no or unknown baseline CNS metastases, the primary endpoint was CNS disease-free survival (CNS-DFS; time from osimertinib start until occurrence of new CNS metastases). Relationships between SNPs and baseline characteristics with CNS-PFS and CNS-DFS were studied with competing-risks survival analysis. Secondary endpoints were relationships between SNPs and PFS, overall survival, severe toxicity, and osimertinib pharmacokinetics.
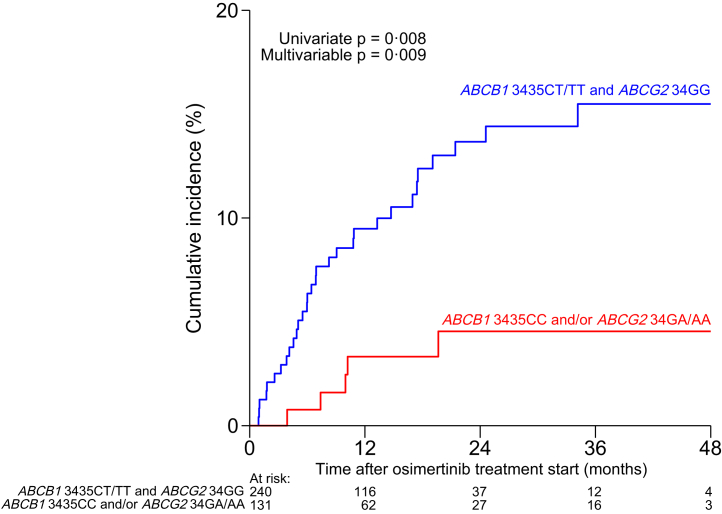
From 572 included patients, 201 had baseline CNS metastases. No SNP was associated with CNS-PFS. Genotype 34GA/AA and/or 3435CC --present in 35% of patients-- was significantly associated with decreased CNS-DFS (hazard ratio 0.28; 95% CI 0.11-0.73; p = 0.009) in the multivariate analysis. This remained significant after applying a Bonferroni correction and internal validation through bootstrapping. 421CA/AA was related to more severe toxicity (27.0% versus 16.5%; p = 0.010).
ABCG2 34G>A and 3435C>T are predictors for developing new CNS metastases during osimertinib treatment, probably because of diminished drug levels in the CNS. 421C>A was significantly related with the incidence of severe toxicity. Pre-emptive genotyping for these SNPs could individualize osimertinib therapy. Addition of ABCG2 inhibitors for patients without 34G>A should be studied further, to prevent new CNS metastases during osimertinib treatment.
No funding was received for this trial.
在转移性表皮生长因子受体突变(m+)的非小细胞肺癌(NSCLC)患者中,约40%存在中枢神经系统(CNS)转移。表皮生长因子受体酪氨酸激酶抑制剂奥希替尼是转运蛋白ABCB1和ABCG2的底物,并由CYP3A4代谢。我们研究了单核苷酸多态性(SNP)3435C>T、421C>A和34G>A与奥希替尼在m+ NSCLC患者中的中枢神经系统治疗疗效之间的关系。
本回顾性观察性多中心队列研究纳入了2014年11月至2021年6月期间开始使用奥希替尼治疗m+ NSCLC的患者。对于有基线中枢神经系统转移的患者,主要终点是中枢神经系统无进展生存期(CNS-PFS;从开始使用奥希替尼到中枢神经系统疾病进展或死亡的时间)。对于无或基线中枢神经系统转移情况未知的患者,主要终点是中枢神经系统无病生存期(CNS-DFS;从开始使用奥希替尼到出现新的中枢神经系统转移的时间)。采用竞争风险生存分析研究SNP与中枢神经系统无进展生存期和中枢神经系统无病生存期的基线特征之间的关系。次要终点是SNP与无进展生存期、总生存期、严重毒性和奥希替尼药代动力学之间的关系。
在纳入的572例患者中,201例有基线中枢神经系统转移。没有SNP与中枢神经系统无进展生存期相关。在多变量分析中,35%的患者存在的基因型34GA/AA和/或3435CC与中枢神经系统无病生存期降低显著相关(风险比0.28;95%置信区间0.11 - 0.73;p = 0.009)。在应用Bonferroni校正并通过自抽样进行内部验证后,这一结果仍然显著。421CA/AA与更严重的毒性相关(27.0%对16.5%;p = 0.010)。
ABCG2 34G>A和3435C>T是奥希替尼治疗期间发生新的中枢神经系统转移的预测指标,可能是由于中枢神经系统中的药物水平降低。421C>A与严重毒性的发生率显著相关。对这些SNP进行前瞻性基因分型可以使奥希替尼治疗个体化。对于没有34G>A的患者,应进一步研究添加ABCG2抑制剂,以预防奥希替尼治疗期间新的中枢神经系统转移。
本试验未获得资金支持。