School of Medicine, University of Leeds, Leeds, UK.
Institute of Cardiovascular and Medical Sciences, College of Medical, Veterinary and Life Sciences, University of Glasgow, Glasgow, UK.
Open Heart. 2023 May;10(1). doi: 10.1136/openhrt-2022-002221.
Guidelines for suspected cardiac chest pain have used historical risk stratification tools, advocating invasive coronary angiography (ICA) first-line in those at highest risk. We aimed to determine whether different strategies to manage suspected stable angina affected medium-term cardiovascular event rates and patient-reported quality of life (QoL) measures.
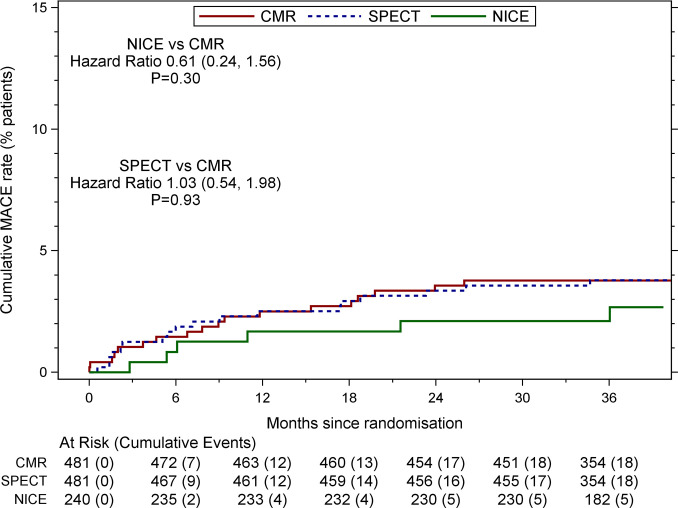
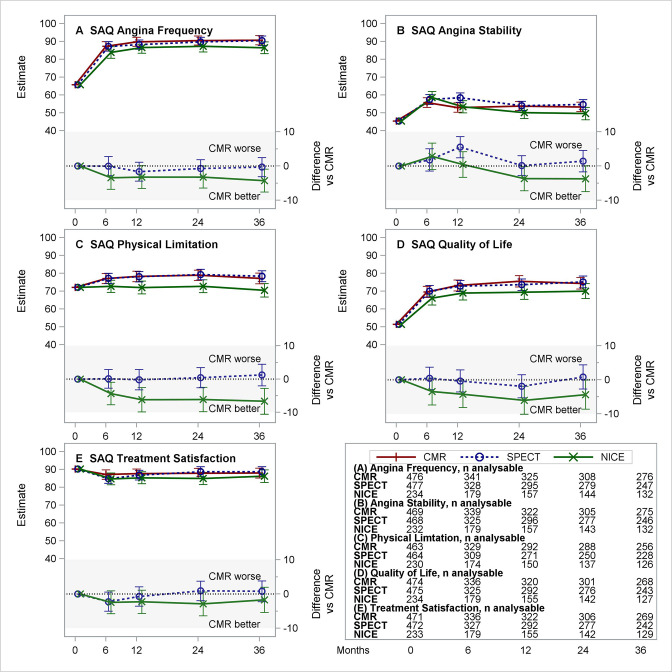
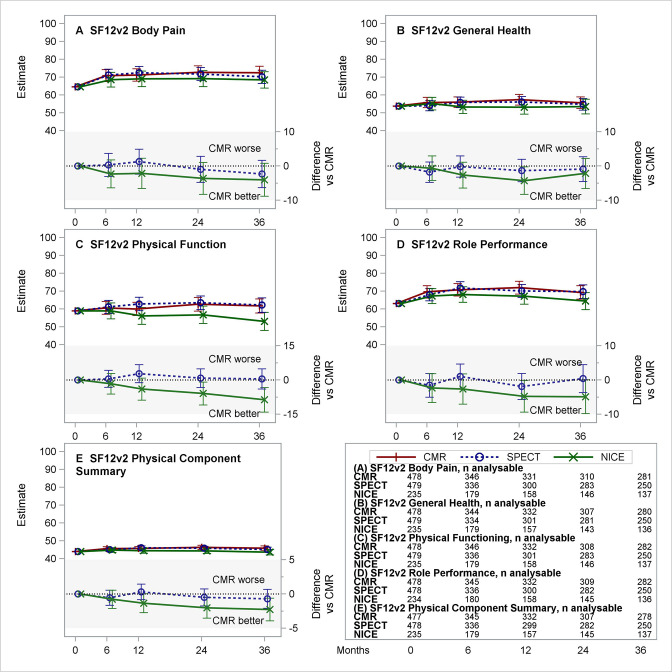
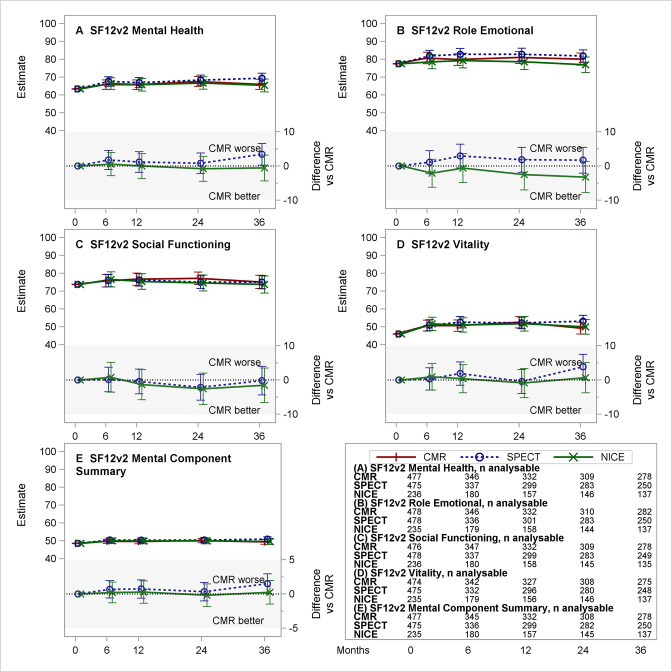
CE-MARC 2, a three-arm parallel group trial, randomised patients with suspected stable cardiac chest pain and a Duke Clinical pretest likelihood of coronary artery disease between 10% and 90%. Patients were randomised to either first-line cardiovascular magnetic resonance (CMR), single-photon emission computed tomography (SPECT) or the UK National Institute for Health and Care Excellence (NICE) CG95 (2010) guidelines-directed care. For the three arms, 1-year and 3-year first major adverse cardiovascular event (MACE) rates and QoL assessed by the Seattle Angina Questionnaire, Short Form 12 (V.12) Questionnaire and EuroQol-5 Dimension Questionnaire were recorded.
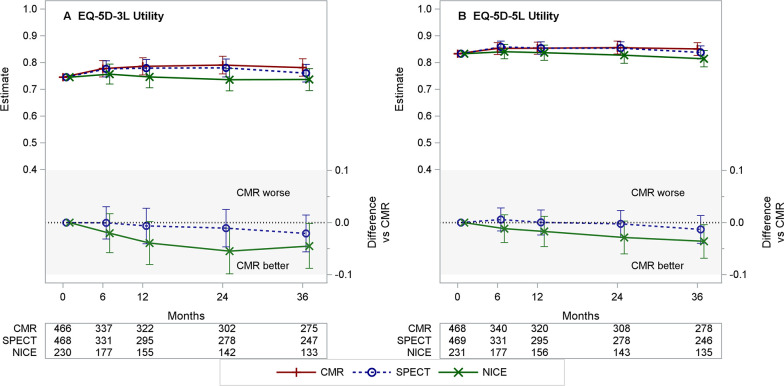
1202 patients were randomised to CMR (n=481), SPECT (n=481) and NICE (n=240). Forty-two patients (18 CMR, 18 SPECT, 6 NICE) experienced one or more MACEs. The percentage rates (95% CIs) of MACE in the CMR, SPECT and NICE groups at 3 years were 3.7% (2.4%, 5.8%), 3.7% (2.4%, 5.8%) and 2.1% (0.9%, 4.8%), respectively. QoL scores did not significantly differ across domains.
Despite a fourfold increase in referrals for ICA, the NICE CG95 (2010) guidelines risk-stratified care strategy did not significantly reduce 3-year MACE or improve QoL, as compared with functional imaging with CMR or SPECT.
ClinicalTrials.gov Registry (NCT01664858).
疑似心脏胸痛的指南使用了历史风险分层工具,主张对风险最高的患者首先进行有创性冠状动脉造影(ICA)。我们旨在确定管理疑似稳定型心绞痛的不同策略是否会影响中期心血管事件发生率和患者报告的生活质量(QoL)测量。
CE-MARC 2 是一项三臂平行组试验,对疑似稳定型心脏胸痛和 Duke 临床预测试验冠心病可能性在 10%至 90%之间的患者进行随机分组。患者随机分配到一线心血管磁共振(CMR)、单光子发射计算机断层扫描(SPECT)或英国国家卫生与保健卓越研究所(NICE)CG95(2010)指南指导的护理。对于这三个组,记录了 1 年和 3 年的首次主要不良心血管事件(MACE)发生率和西雅图心绞痛问卷、简短形式 12(V.12)问卷和 EuroQol-5 维度问卷评估的 QoL。
1202 名患者被随机分配到 CMR(n=481)、SPECT(n=481)和 NICE(n=240)组。42 名患者(18 名 CMR、18 名 SPECT、6 名 NICE)发生了 1 次或多次 MACE。CMR、SPECT 和 NICE 组在 3 年内的 MACE 百分比(95%CI)分别为 3.7%(2.4%,5.8%)、3.7%(2.4%,5.8%)和 2.1%(0.9%,4.8%)。各领域的 QoL 评分没有显著差异。
尽管 ICA 的转诊率增加了四倍,但与 CMR 或 SPECT 的功能成像相比,NICE CG95(2010)指南风险分层护理策略并不能显著降低 3 年 MACE 发生率或改善 QoL。
ClinicalTrials.gov 注册表(NCT01664858)。