Department of Psychology, Center for Human Sleep Science, University of California Berkeley, Berkeley, CA, 94720, USA.
Department of Psychiatry and Human Behavior, University of California, Irvine, CA, 92617, USA.
BMC Med. 2023 May 3;21(1):156. doi: 10.1186/s12916-023-02811-z.
Alzheimer's disease (AD) pathology impairs cognitive function. Yet some individuals with high amounts of AD pathology suffer marked memory impairment, while others with the same degree of pathology burden show little impairment. Why is this? One proposed explanation is cognitive reserve i.e., factors that confer resilience against, or compensation for the effects of AD pathology. Deep NREM slow wave sleep (SWS) is recognized to enhance functions of learning and memory in healthy older adults. However, that the quality of NREM SWS (NREM slow wave activity, SWA) represents a novel cognitive reserve factor in older adults with AD pathology, thereby providing compensation against memory dysfunction otherwise caused by high AD pathology burden, remains unknown.
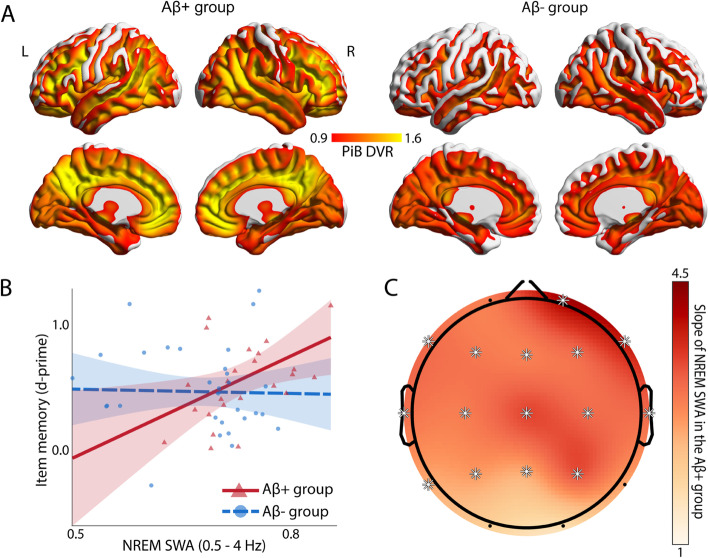
Here, we tested this hypothesis in cognitively normal older adults (N = 62) by combining C-PiB (Pittsburgh compound B) positron emission tomography (PET) scanning for the quantification of β-amyloid (Aβ) with sleep electroencephalography (EEG) recordings to quantify NREM SWA and a hippocampal-dependent face-name learning task.
We demonstrated that NREM SWA significantly moderates the effect of Aβ status on memory function. Specifically, NREM SWA selectively supported superior memory function in individuals suffering high Aβ burden, i.e., those most in need of cognitive reserve (B = 2.694, p = 0.019). In contrast, those without significant Aβ pathological burden, and thus without the same need for cognitive reserve, did not similarly benefit from the presence of NREM SWA (B = -0.115, p = 0.876). This interaction between NREM SWA and Aβ status predicting memory function was significant after correcting for age, sex, Body Mass Index, gray matter atrophy, and previously identified cognitive reserve factors, such as education and physical activity (p = 0.042).
These findings indicate that NREM SWA is a novel cognitive reserve factor providing resilience against the memory impairment otherwise caused by high AD pathology burden. Furthermore, this cognitive reserve function of NREM SWA remained significant when accounting both for covariates, and factors previously linked to resilience, suggesting that sleep might be an independent cognitive reserve resource. Beyond such mechanistic insights are potential therapeutic implications. Unlike many other cognitive reserve factors (e.g., years of education, prior job complexity), sleep is a modifiable factor. As such, it represents an intervention possibility that may aid the preservation of cognitive function in the face of AD pathology, both present moment and longitudinally.
阿尔茨海默病(AD)病理学损害认知功能。然而,一些患有大量 AD 病理学的人遭受明显的记忆障碍,而其他具有相同程度病理学负担的人则几乎没有受到影响。为什么会这样?一种提出的解释是认知储备,即赋予对 AD 病理学的影响产生抵抗力或补偿的因素。深度非快速眼动慢波睡眠(SWS)被认为可以增强健康老年人的学习和记忆功能。然而,非快速眼动 SWS 的质量(非快速眼动慢波活动,SWA)是否代表 AD 病理学患者的一种新的认知储备因素,从而对因 AD 病理学负担高而引起的记忆功能障碍提供补偿,目前尚不清楚。
在这里,我们通过结合 C-PiB(匹兹堡化合物 B)正电子发射断层扫描(PET)扫描来定量β-淀粉样蛋白(Aβ),并结合睡眠脑电图(EEG)记录来定量非快速眼动 SWA 和海马依赖的面孔-名称学习任务,对认知正常的老年人(N = 62)进行了测试。
我们证明,非快速眼动 SWA 显著调节 Aβ状态对记忆功能的影响。具体来说,非快速眼动 SWA 选择性地支持 Aβ负担高的个体的记忆功能,即最需要认知储备的个体(B = 2.694,p = 0.019)。相比之下,那些没有显著的 Aβ病理负担,因此没有相同的认知储备需求的个体,并没有从非快速眼动 SWA 的存在中得到类似的益处(B = -0.115,p = 0.876)。在对年龄、性别、体重指数、灰质萎缩和先前确定的认知储备因素(如教育和体育活动)进行校正后,这种非快速眼动 SWA 与 Aβ状态预测记忆功能之间的相互作用具有统计学意义(p = 0.042)。
这些发现表明,非快速眼动 SWA 是一种新的认知储备因素,为因 AD 病理学负担高而引起的记忆障碍提供了恢复能力。此外,当考虑到协变量和与恢复力相关的因素时,这种非快速眼动 SWA 的认知储备功能仍然具有统计学意义,这表明睡眠可能是一种独立的认知储备资源。除了这些机制上的见解之外,还有潜在的治疗意义。与许多其他认知储备因素(如受教育年限、先前工作复杂性)不同,睡眠是一个可调节的因素。因此,它代表了一种干预可能性,可能有助于在 AD 病理学存在的情况下维持认知功能,无论是现在还是长远。