Lecturer, Department of Orthodontics, Faculty of Dentistry, Alexandria University, Champolion Street, Alexandria, El Azarita, Egypt.
PhD resident, Department of Orthodontics, Faculty of Dentistry, Alexandria University, Alexandria, Egypt.
BMC Oral Health. 2023 May 3;23(1):260. doi: 10.1186/s12903-023-02940-0.
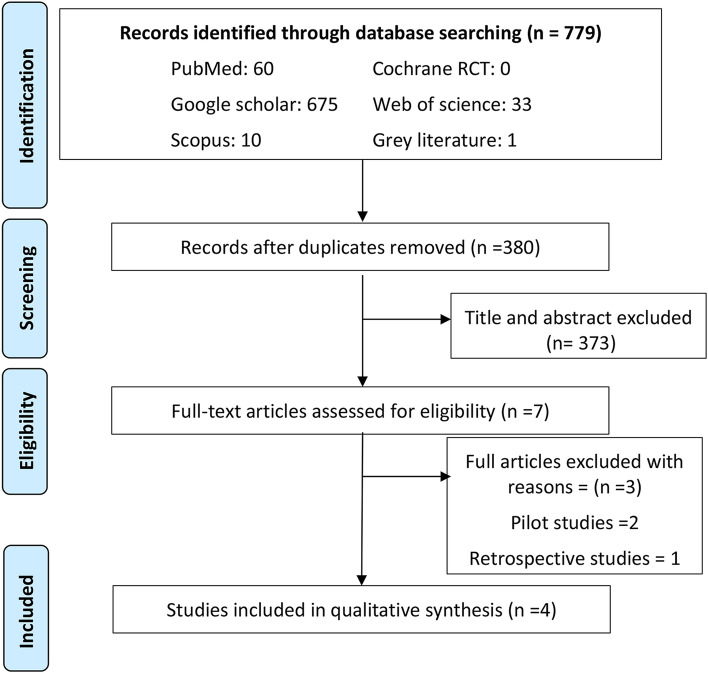
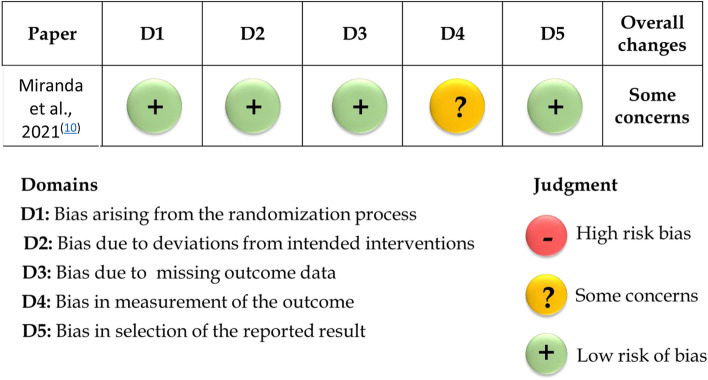
The introduction of skeletal anchorage utilized for maxillary protraction with a face mask or class III elastics has been developed for the management of class III malocclusions with minimal dental effect. The objective of the present review was to evaluate the current evidence regarding airway dimensional changes following bone-anchored maxillary protraction. A search was conducted by two authors (S.A & B.A) in the following databases: MEDLINE via PubMed, Cochrane Library, Web of Science, Scopus, Google Scholar and Open Grey; besides a hand search in references of selected articles and developing a search alert in electronic databases. Selection criteria comprised randomized as well as prospective clinical trials evaluating airway dimensional changes following bone-anchored maxillary protraction. Relevant data were extracted after studies retrieval and selection. The risk of bias was thereafter evaluated using the revised RoB 2 tool for randomized clinical trials and the ROBINS-I tool was used for non-randomized clinical trials. The quality of studies was assessed using the modified Jadad score. After examining (eligibility) full-text articles, four clinical trials were ultimately included. These studies evaluated the airway dimensional changes, following bone-anchored maxillary protraction in comparison to different control study groups. Based on the available evidence, all the bone-anchored maxillary protraction devices used in the eligible studies in the present systematic review resulted in an improvement in the airway dimensions. However, due to the few numbers of studies available and the guarded evidence due to the low quality of evidence of three out of four included articles, there is no strong evidence to support a significant increase in the airway dimensions following bone-anchored maxillary protraction. Therefore, there is a need for more randomized controlled clinical trials with similar bone-anchored protraction devices and similar assessment methods for more valid comparisons, excluding any confounding factors, on airway dimensional changes.
引入利用面弓或 III 类橡皮筋的骨骼锚固来进行上颌前牵引,是为了在最小的牙齿影响下管理 III 类错颌畸形。本综述的目的是评估目前关于骨锚定上颌前牵引后气道尺寸变化的证据。两位作者(S.A 和 B.A)在以下数据库中进行了搜索:MEDLINE 通过 PubMed、Cochrane 图书馆、Web of Science、Scopus、Google Scholar 和 Open Grey;此外,还对手头选定文章的参考文献进行了搜索,并在电子数据库中开发了搜索警报。选择标准包括评价骨锚定上颌前牵引后气道尺寸变化的随机对照临床试验以及前瞻性临床试验。在研究检索和选择后提取相关数据。然后使用修订后的 RoB 2 工具评估随机临床试验的偏倚风险,使用 ROBINS-I 工具评估非随机临床试验的偏倚风险。使用改良 Jadad 评分评估研究质量。在检查(合格性)全文文章后,最终纳入了四项临床试验。这些研究评估了骨锚定上颌前牵引与不同对照组相比的气道尺寸变化。根据现有证据,本系统评价中纳入的所有合格研究中使用的骨锚定上颌前牵引装置均导致气道尺寸改善。然而,由于研究数量较少,并且由于四篇纳入文章中有三篇的证据质量较低,因此证据质量存在一定的局限性,无法有力地支持骨锚定上颌前牵引后气道尺寸显著增加。因此,需要更多具有类似骨锚定前牵引装置和类似评估方法的随机对照临床试验,以排除任何混杂因素,对气道尺寸变化进行更有效的比较。