Borges Ana Paula, Antunes Célia, Caseiro-Alves Filipe, Donato Paulo
Radiology Department, Coimbra Hospital and Universitary Centre, Praceta Professor Mota Pinto, 3004-561, Coimbra, Portugal.
Faculty of Medicine of the University of Coimbra, Rua Larga 2, 3000-370, Coimbra, Portugal.
Thyroid Res. 2023 May 8;16(1):12. doi: 10.1186/s13044-023-00155-7.
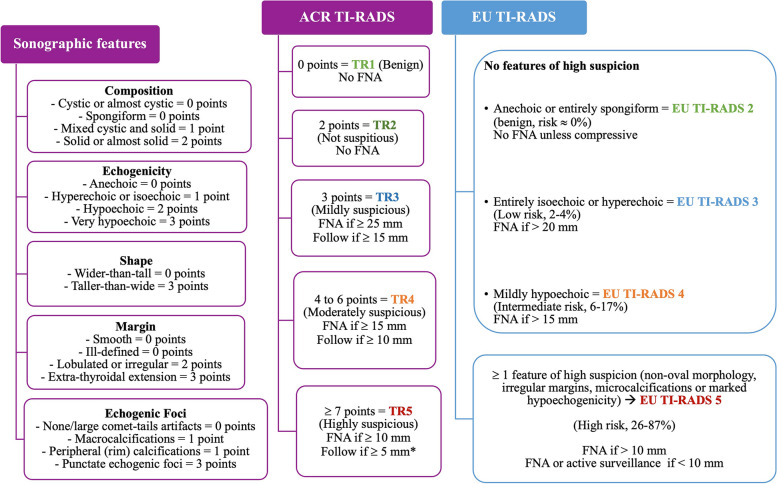
Ultrasound-based classification systems allow stratification of thyroid nodules to recommend fine-needle aspiration (FNA) based on their malignancy risk. However, these have discrepancies that may have an impact in thyroid cancer detection. We aimed to compare European Thyroid Association (EU-TIRADS) and American College of Radiology (ACR TI-RADS), in terms of FNA indication and diagnostic performance.
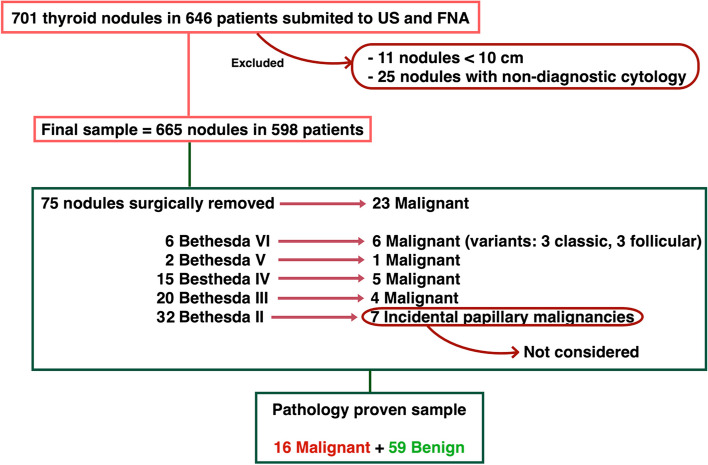
Retrospective study of 665 thyroid nodules from 598 patients who underwent ultrasound and fine-needle aspiration at a tertiary-care institution between January 1 of 2016 and July 31 of 2019. Based on their sonographic features they were classified according to the EU-TIRADS and ACR TI-RADS classification and then their cytological results were obtained. Differences in FNA indications according to these two classifications were analysed. In patients who underwent surgical removal of the nodules, the final pathological diagnosis was obtained.
A statistically significant association was found between EU-TIRADS and ACR TI-RADS classification systems (p < 0.001). ACR TI-RADS allowed greatest reduction in FNA performed (32% vs 24.5%). A different risk category was obtained in 174 (26.1%) nodules, mostly higher with EU-TIRADS. The indication to FNA changed in 54 (8.1%) nodules (49 only indicated following EU-TIRADS recommendations), of which 4 had Bethesda IV and 5 had Bethesda III cytology. The FNA indication in a higher number of nodules using EU-TIRADS was due to difference in the dimensional threshold for FNA on low-risk nodules; to the fact that hypoechogenicity in a mixed nodule ascribes it moderate risk, while using ACR TI-RADS it would only be considered of low risk, and to the use of isolated sonographic features, namely marked hypoechogenicity, microcalcifications and irregular margins, to automatically categorize a nodules as high risk in EU-TIRADS, while ACR TI-RADS requires a group of potentially suspicious features to consider a nodule of high risk. The analysis of pathology proven nodules revealed equally good sensitivity of both systems in the detection of malignancy, but weak specificity, slightly greater with ACR TI-RADS (27.1% vs 18.6%).
The EU-TIRADS and ACR TI-RADS are both suitable to assess thyroid nodules and through risk stratification avoid unnecessary FNA. FNA was less performed using ACR TI-RADS, which was slightly more efficiency in excluding malignancy.
基于超声的分类系统可根据甲状腺结节的恶性风险对其进行分层,以推荐细针穿刺活检(FNA)。然而,这些系统存在差异,可能会对甲状腺癌的检测产生影响。我们旨在比较欧洲甲状腺协会(EU-TIRADS)和美国放射学会(ACR TI-RADS)在FNA指征和诊断性能方面的差异。
对2016年1月1日至2019年7月31日期间在一家三级医疗机构接受超声检查和细针穿刺活检的598例患者的665个甲状腺结节进行回顾性研究。根据超声特征,按照EU-TIRADS和ACR TI-RADS分类进行分类,然后获取其细胞学结果。分析这两种分类方法在FNA指征上的差异。对于接受结节手术切除的患者,获取最终病理诊断结果。
发现EU-TIRADS和ACR TI-RADS分类系统之间存在统计学显著关联(p < 0.001)。ACR TI-RADS使进行FNA的比例降幅最大(32%对24.5%)。174个(26.1%)结节获得了不同的风险类别,大多数情况下EU-TIRADS的风险类别更高。54个(8.1%)结节的FNA指征发生了变化(49个仅在遵循EU-TIRADS建议后才进行FNA),其中4个为贝塞斯达IV类,5个为贝塞斯达III类细胞学结果。使用EU-TIRADS时更多结节有FNA指征,原因在于低风险结节FNA的尺寸阈值存在差异;混合性结节中的低回声使其被归类为中度风险,而使用ACR TI-RADS时仅被视为低风险;以及在EU-TIRADS中使用孤立的超声特征,即显著低回声、微钙化和边缘不规则,将结节自动归类为高风险,而ACR TI-RADS需要一组潜在可疑特征才将结节视为高风险。对病理证实的结节进行分析发现,两种系统在检测恶性肿瘤方面的敏感性相同,但特异性较弱,ACR TI-RADS的特异性略高(27.1%对18.6%)。
EU-TIRADS和ACR TI-RADS都适用于评估甲状腺结节,并通过风险分层避免不必要的FNA。使用ACR TI-RADS时进行FNA的情况较少,并在排除恶性肿瘤方面效率略高。