Lage Luís Alberto de Pádua Covas, Culler Hebert Fabricio, Reichert Cadiele Oliana, da Siqueira Sheila Aparecida Coelho, Pereira Juliana
Department of Hematology, Hemotherapy & Cell Therapy, University of São Paulo (USP), São Paulo, SP, Brazil.
Laboratory of Medical Investigation in Pathogenesis and Directed Therapy in Onco-Immuno-Hematology (LIM-31), University of São Paulo (USP), São Paulo, SP, Brazil.
Front Oncol. 2023 Apr 26;13:1177590. doi: 10.3389/fonc.2023.1177590. eCollection 2023.
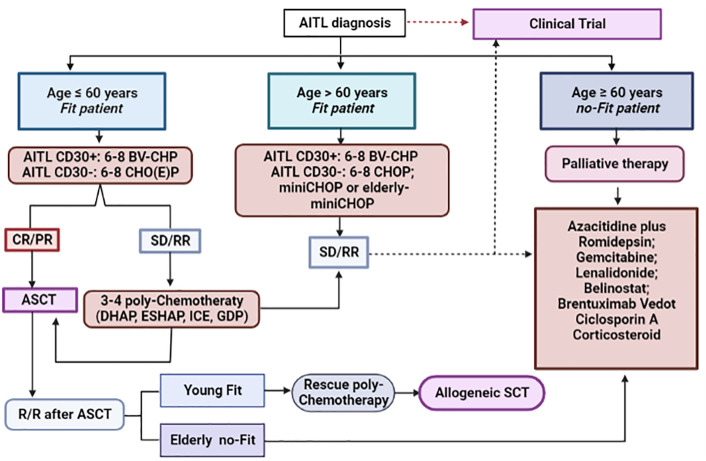
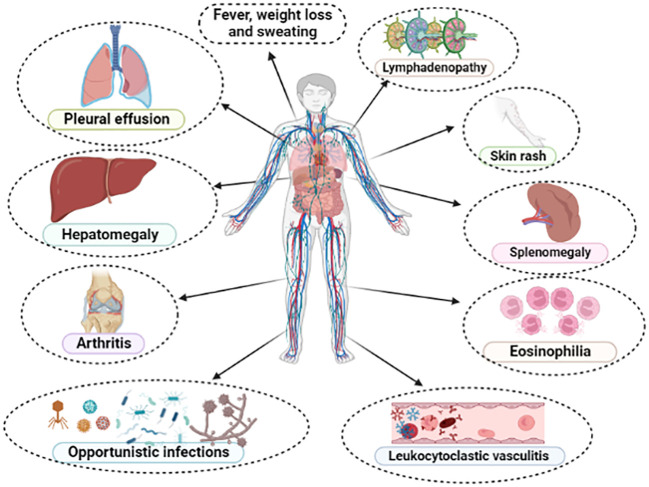
Angioimmunoblastic T-cell lymphoma (AITL) is the second most frequent subtype of mature T-cell lymphoma (MTCL) in the Western world. It derives from the monoclonal proliferation of T-follicular helper (TFH) cells and is characterized by an exacerbated inflammatory response and immune dysregulation, with predisposition to autoimmunity phenomena and recurrent infections. Its genesis is based on a multistep integrative model, where age-related and initiator mutations involve epigenetic regulatory genes, such as and . Subsequently, driver-mutations, such as G17V and R172K/S promote the expansion of clonal TFH-cells ("second-hit"), that finally begin to secrete cytokines and chemokines, such as IL-6, IL-21, CXCL-13 and VEGF, modulating a network of complex relationships between TFH-cells and a defective tumor microenvironment (TME), characterized by expansion of follicular dendritic cells (FDC), vessels and EBV-positive immunoblasts. This unique pathogenesis leads to peculiar clinical manifestations, generating the so-called "", typical of AITL. Its differential diagnosis is broad, involving viral infections, collagenosis and adverse drug reactions, which led many authors to use the term "" when referring to AITL. Although great advances in its biological knowledge have been obtained in the last two decades, its treatment is still an unmet medical need, with highly reserved clinical outcomes. Outside the setting of clinical trials, AITL patients are still treated with multidrug therapy based on anthracyclines (CHOP-like), followed by up-front consolidation with autologous stem cell transplantation (ASCT). In this setting, the estimated 5-year overall survival (OS) is around 30-40%. New drugs, such as hypomethylating agents (HMAs) and histone deacetylase inhibitors (HDAi), have been used for relapsed/refractory (R/R) disease with promising results. Such agents have their use based on a biological rationale, have significant potential to improve the outcomes of patients with AITL and may represent a paradigm shift in the therapeutic approach to this lymphoma in the near future.
血管免疫母细胞性T细胞淋巴瘤(AITL)是西方世界中成熟T细胞淋巴瘤(MTCL)的第二常见亚型。它起源于T滤泡辅助(TFH)细胞的单克隆增殖,其特征是炎症反应加剧和免疫失调,易发生自身免疫现象和反复感染。其发生基于一个多步骤整合模型,其中与年龄相关的起始突变涉及表观遗传调控基因,如 和 。随后,驱动突变,如 G17V和 R172K/S促进克隆性TFH细胞的扩增(“二次打击”),最终这些细胞开始分泌细胞因子和趋化因子,如IL-6、IL-21、CXCL-13和VEGF,调节TFH细胞与有缺陷的肿瘤微环境(TME)之间的复杂关系网络,该微环境的特征是滤泡树突状细胞(FDC)、血管和EBV阳性免疫母细胞的扩增。这种独特的发病机制导致了特殊的临床表现,产生了所谓的“AITL特征性表现”。其鉴别诊断范围广泛,涉及病毒感染、胶原病和药物不良反应,这使得许多作者在提及AITL时使用“假性淋巴瘤”一词。尽管在过去二十年中对其生物学知识有了很大进展,但其治疗仍然是未满足的医疗需求,临床结果很不理想。在临床试验之外,AITL患者仍接受基于蒽环类药物的多药治疗(CHOP样方案),随后进行自体干细胞移植(ASCT)的前期巩固治疗。在这种情况下,估计5年总生存率(OS)约为30%-40%。新药,如低甲基化剂(HMAs)和组蛋白去乙酰化酶抑制剂(HDAi),已用于复发/难治性(R/R)疾病并取得了有希望的结果。这些药物基于生物学原理使用,有显著潜力改善AITL患者的预后,并且在不久的将来可能代表这种淋巴瘤治疗方法的范式转变。