Department of Pathology, Forensic and Insurance Medicine, Semmelweis University, Üllői út 93, 1091, Budapest, Hungary.
Department of Surgery, Leiden University Medical Centre, Albinusdreef 2, 2333 ZA, Leiden, The Netherlands.
Virchows Arch. 2024 Oct;485(4):703-716. doi: 10.1007/s00428-023-03555-0. Epub 2023 May 18.
Tumour-stroma ratio (TSR) is an important prognostic and predictive factor in several tumour types. The aim of this study is to determine whether TSR evaluated in breast cancer core biopsies is representative of the whole tumour.
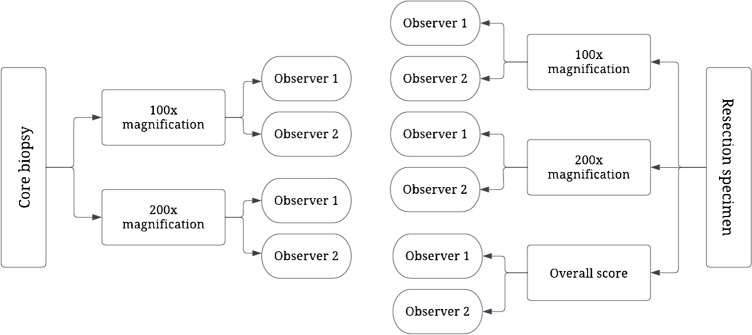
Different TSR scoring methods, their reproducibility, and the association of TSR with clinicopathological characteristics were investigated in 178 breast carcinoma core biopsies and corresponding resection specimens. TSR was assessed by two trained scientists on the most representative H&E-stained digitised slides. Patients were treated primarily with surgery between 2010 and 2021 at Semmelweis University, Budapest.
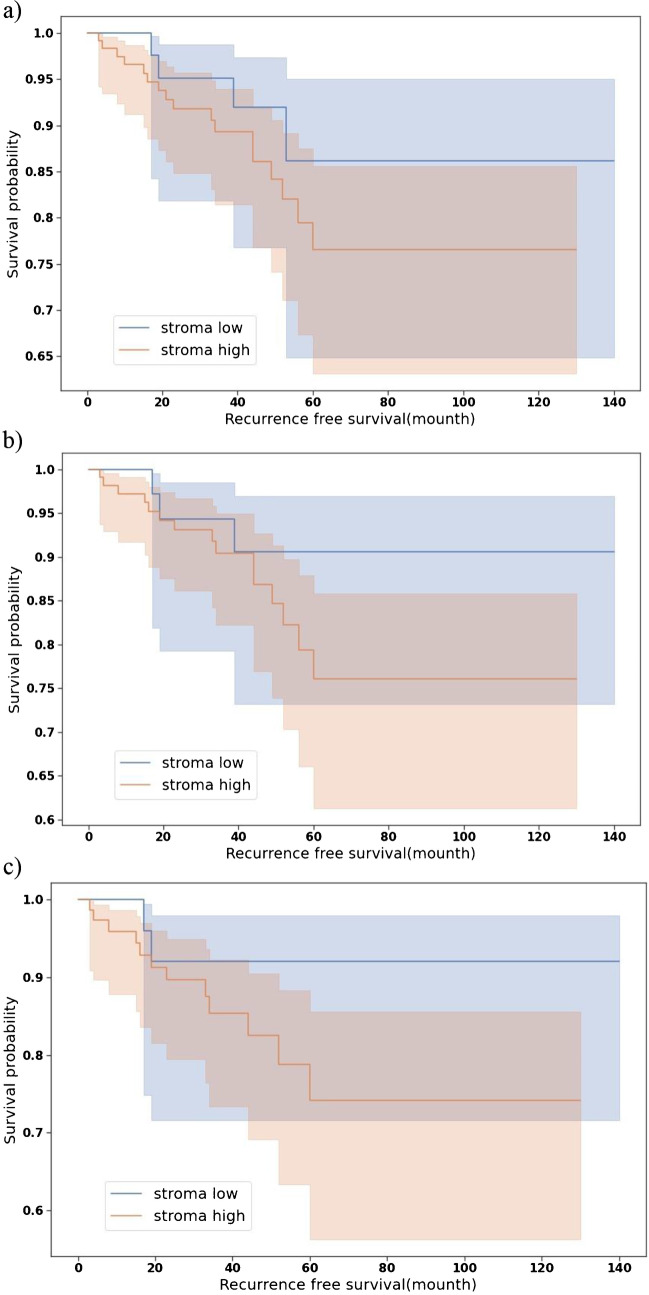
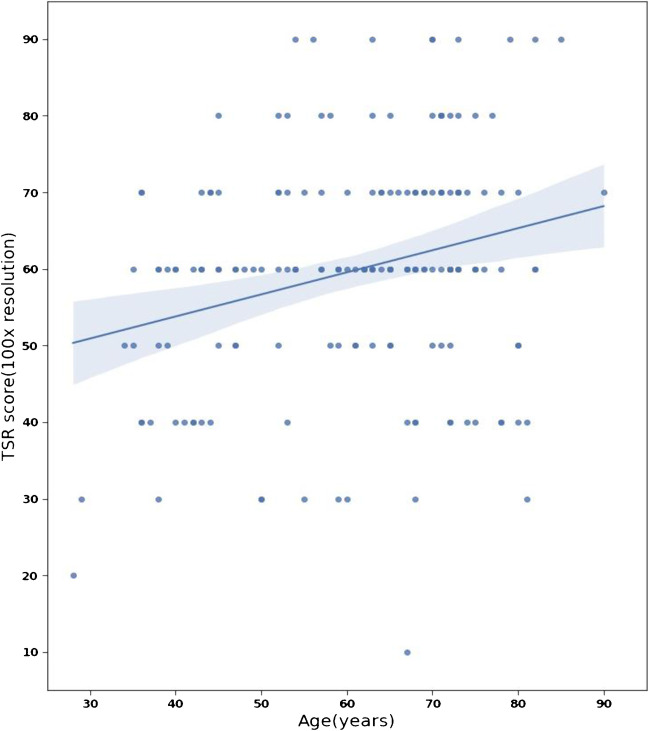
Ninety-one percent of the tumours were hormone receptor (HR)-positive (luminal-like). Interobserver agreement was highest using 100 × magnification (κ = 0.906, κ = 0.882). The agreement between TSR of core biopsies and resection specimens of the same patients was moderate (κ = 0.514). Differences between the two types of samples were most frequent in cases with TSR scores close to the 50% cut-off point. TSR was strongly correlated with age at diagnosis, pT category, histological type, histological grade, and surrogate molecular subtype. A tendency was identified for more recurrences among stroma-high (SH) tumours (p = 0.07). Significant correlation was detected between the TSR and tumour recurrence in grade 1 HR-positive breast cancer cases (p = 0.03).
TSR is easy to determine and reproducible on both core biopsies and in resection specimens and is associated with several clinicopathological characteristics of breast cancer. TSR scored on core biopsies is moderately representative for the whole tumour.
肿瘤间质比(TSR)是几种肿瘤类型的重要预后和预测因素。本研究旨在确定在乳腺癌核心活检中评估的 TSR 是否代表整个肿瘤。
在 178 例乳腺癌核心活检和相应的切除标本中,研究了不同的 TSR 评分方法、其可重复性以及 TSR 与临床病理特征的相关性。两位经过培训的科学家在最具代表性的 H&E 染色数字化切片上评估 TSR。患者于 2010 年至 2021 年在布达佩斯塞梅尔维斯大学接受了主要的手术治疗。
91%的肿瘤为激素受体(HR)阳性(腔型样)。使用 100×放大倍数时,观察者间的一致性最高(κ=0.906,κ=0.882)。核心活检与同一患者的切除标本之间的一致性为中度(κ=0.514)。在接近 50%截断点的 TSR 评分的情况下,两种类型的样本之间的差异最为频繁。TSR 与诊断时的年龄、pT 类别、组织学类型、组织学分级和替代分子亚型强烈相关。在间质高(SH)肿瘤中,复发的趋势更为明显(p=0.07)。在 HR 阳性 1 级乳腺癌病例中,TSR 与肿瘤复发之间存在显著相关性(p=0.03)。
TSR 易于在核心活检和切除标本上确定且具有可重复性,与乳腺癌的多个临床病理特征相关。核心活检上的 TSR 评分对整个肿瘤具有中等代表性。