Jamal Nadim E, Brooks Thomas G, Cohen Jordana, Townsend Raymond R, de Sosa Giselle Rodriguez, Shah Vallabh, Nelson Robert G, Drawz Paul E, Rao Panduranga, Bhat Zeenat, Chang Alexander, Yang Wei, FitzGerald Garret A, Skarke Carsten
Institute for Translational Medicine and Therapeutics (ITMAT), University of Pennsylvania Perelman School of Medicine, Philadelphia, PA, USA.
Renal-Electrolyte and Hypertension Division, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA, USA.
medRxiv. 2023 May 5:2023.05.02.23289413. doi: 10.1101/2023.05.02.23289413.
Chronic kidney disease (CKD) represents a significant global burden. Hypertension is a modifiable risk factor for rapid progression of CKD.
We extend the risk stratification by introducing the non-parametric determination of rhythmic components in 24-hour profiles of ambulatory blood pressure monitoring (ABPM) in the African American Study for Kidney Disease and Hypertension (AASK) cohort and the Chronic Renal Insufficiency Cohort (CRIC) using Cox proportional hazards models.
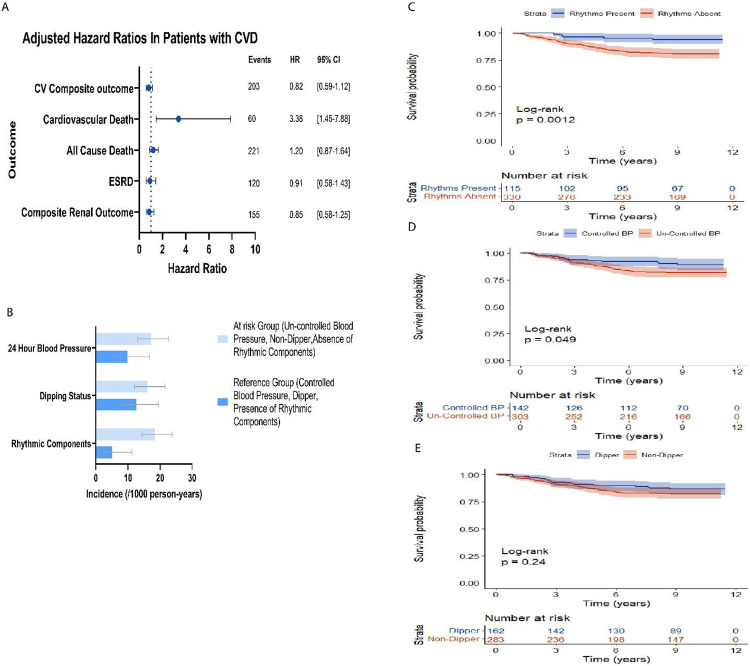
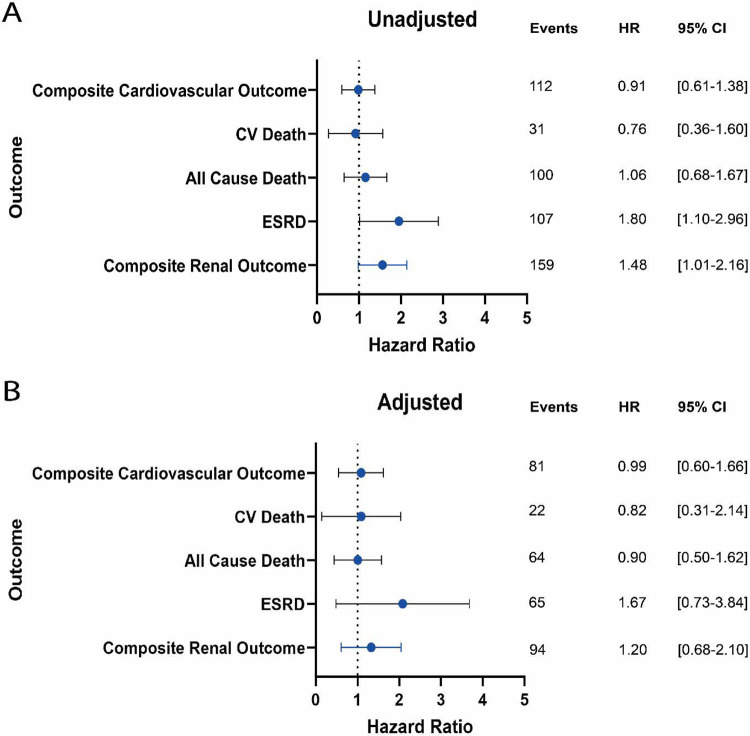
We find that rhythmic profiling of BP through JTK_Cycle analysis identifies subgroups of CRIC participants at advanced risk of cardiovascular death. CRIC participants with a history of cardiovascular disease (CVD) and absent cyclic components in their BP profile had at any time a 3.4-times higher risk of cardiovascular death than CVD patients with cyclic components present in their BP profile (HR: 3.38, 95% CI: 1.45-7.88, =0.005). This substantially increased risk was independent of whether ABPM followed a dipping or non-dipping pattern whereby non-dipping or reverse dipping were not significantly associated with cardiovascular death in patients with prior CVD (>0.1). In the AASK cohort, unadjusted models demonstrate a higher risk in reaching end stage renal disease among participants without rhythmic ABPM components (HR:1.80, 95% CI: 1.10-2.96); however, full adjustment abolished this association.
This study proposes rhythmic blood pressure components as a novel biomarker to unmask excess risk among CKD patients with prior cardiovascular disease.
慢性肾脏病(CKD)是一项重大的全球负担。高血压是CKD快速进展的一个可改变的风险因素。
在非裔美国人肾脏病与高血压研究(AASK)队列和慢性肾功能不全队列(CRIC)中,我们通过使用Cox比例风险模型,在动态血压监测(ABPM)的24小时血压图谱中引入非参数节律成分测定,来扩展风险分层。
我们发现,通过JTK_Cycle分析对血压进行节律分析可识别出CRIC参与者中心血管死亡高风险的亚组。有心血管疾病(CVD)病史且血压图谱中无周期性成分的CRIC参与者在任何时候发生心血管死亡的风险比血压图谱中有周期性成分的CVD患者高3.4倍(风险比:3.38,95%置信区间:1.45 - 7.88,P = 0.005)。这种显著增加的风险与ABPM是勺型还是非勺型模式无关,即非勺型或反勺型与既往有CVD的患者的心血管死亡无显著关联(P>0.1)。在AASK队列中,未经调整的模型显示,无节律性ABPM成分的参与者达到终末期肾病的风险更高(风险比:1.80,95%置信区间:1.10 - 2.96);然而,完全调整后消除了这种关联。
本研究提出将血压节律成分作为一种新型生物标志物,以揭示既往有心血管疾病的CKD患者中的额外风险。