Michi Teresa, Mattana Chiara, Menga Luca S, Bocci Maria Grazia, Cesarano Melania, Rosà Tommaso, Gualano Maria Rosaria, Montomoli Jonathan, Spadaro Savino, Tosato Matteo, Rota Elisabetta, Landi Francesco, Cutuli Salvatore L, Tanzarella Eloisa S, Pintaudi Gabriele, Piervincenzi Edoardo, Bello Giuseppe, Tonetti Tommaso, Rucci Paola, De Pascale Gennaro, Maggiore Salvatore M, Grieco Domenico Luca, Conti Giorgio, Antonelli Massimo
Department of Emergency, Intensive Care Medicine and Anesthesia, Fondazione Policlinico Universitario A. Gemelli IRCCS, L.Go F. Vito, 00168, Rome, Italy.
Istituto Di Anestesiologia E Rianimazione, Catholic University of The Sacred Heart, Rome, Italy.
J Intensive Care. 2023 May 19;11(1):21. doi: 10.1186/s40560-023-00669-0.
Long-term outcomes of patients treated with helmet noninvasive ventilation (NIV) are unknown: safety concerns regarding the risk of patient self-inflicted lung injury and delayed intubation exist when NIV is applied in hypoxemic patients. We assessed the 6-month outcome of patients who received helmet NIV or high-flow nasal oxygen for COVID-19 hypoxemic respiratory failure.
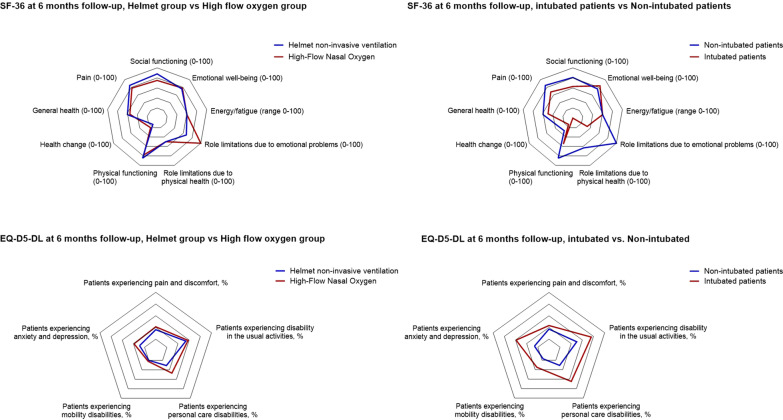
In this prespecified analysis of a randomized trial of helmet NIV versus high-flow nasal oxygen (HENIVOT), clinical status, physical performance (6-min-walking-test and 30-s chair stand test), respiratory function and quality of life (EuroQoL five dimensions five levels questionnaire, EuroQoL VAS, SF36 and Post-Traumatic Stress Disorder Checklist for the DSM) were evaluated 6 months after the enrollment.
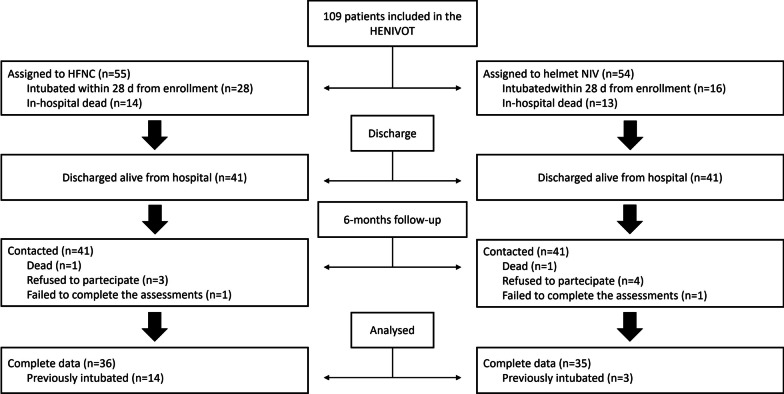
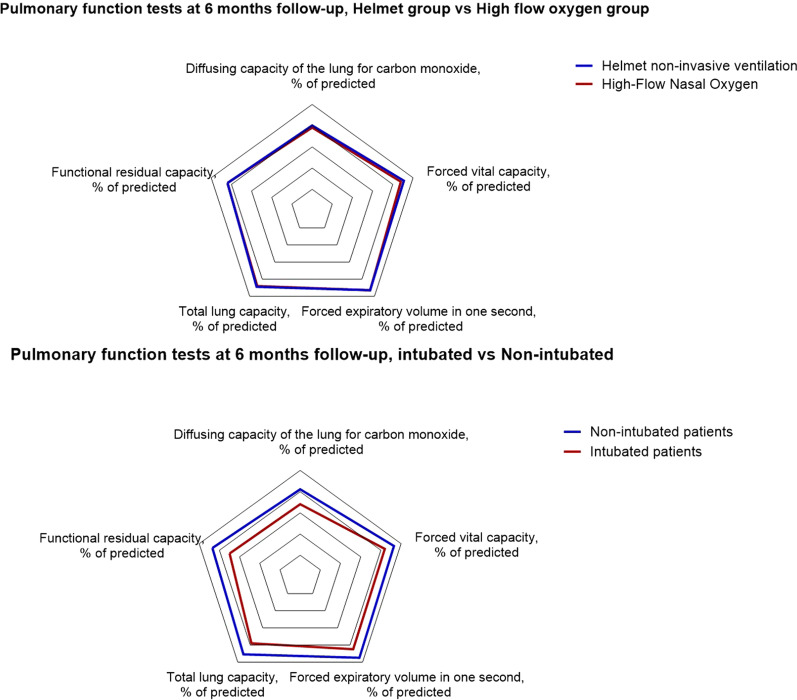
Among 80 patients who were alive, 71 (89%) completed the follow-up: 35 had received helmet NIV, 36 high-flow oxygen. There was no inter-group difference in any item concerning vital signs (N = 4), physical performance (N = 18), respiratory function (N = 27), quality of life (N = 21) and laboratory tests (N = 15). Arthralgia was significantly lower in the helmet group (16% vs. 55%, p = 0.002). Fifty-two percent of patients in helmet group vs. 63% of patients in high-flow group had diffusing capacity of the lungs for carbon monoxide < 80% of predicted (p = 0.44); 13% vs. 22% had forced vital capacity < 80% of predicted (p = 0.51). Both groups reported similar degree of pain (p = 0.81) and anxiety (p = 0.81) at the EQ-5D-5L test; the EQ-VAS score was similar in the two groups (p = 0.27). Compared to patients who successfully avoided invasive mechanical ventilation (54/71, 76%), intubated patients (17/71, 24%) had significantly worse pulmonary function (median diffusing capacity of the lungs for carbon monoxide 66% [Interquartile range: 47-77] of predicted vs. 80% [71-88], p = 0.005) and decreased quality of life (EQ-VAS: 70 [53-70] vs. 80 [70-83], p = 0.01).
In patients with COVID-19 hypoxemic respiratory failure, treatment with helmet NIV or high-flow oxygen yielded similar quality of life and functional outcome at 6 months. The need for invasive mechanical ventilation was associated with worse outcomes. These data indicate that helmet NIV, as applied in the HENIVOT trial, can be safely used in hypoxemic patients. Trial registration Registered on clinicaltrials.gov NCT04502576 on August 6, 2020.
接受头盔无创通气(NIV)治疗的患者的长期预后尚不清楚:在低氧血症患者中应用NIV时,存在患者自我造成肺损伤和延迟插管风险的安全问题。我们评估了接受头盔NIV或高流量鼻导管吸氧治疗新型冠状病毒肺炎(COVID-19)低氧血症呼吸衰竭患者的6个月预后。
在这项头盔NIV与高流量鼻导管吸氧(HENIVOT)随机试验的预设分析中,在入组6个月后评估临床状态、身体功能(6分钟步行试验和30秒坐立试验)、呼吸功能和生活质量(欧洲五维健康量表、欧洲五维视觉模拟量表、SF36和创伤后应激障碍检查表)。
在80名存活患者中,71名(89%)完成了随访:35名接受了头盔NIV,36名接受了高流量吸氧。在任何有关生命体征(N = 4)、身体功能(N = 18)、呼吸功能(N = 27)、生活质量(N = 21)和实验室检查(N = 15)的项目中,两组之间均无差异。头盔组的关节痛明显更低(16% 对55%,p = 0.002)。头盔组52% 的患者与高流量组63% 的患者的肺一氧化碳弥散量低于预测值的80%(p = 0.44);13% 对22% 的患者用力肺活量低于预测值的80%(p = 0.51)。在欧洲五维健康量表-5级(EQ-5D-5L)测试中,两组报告的疼痛程度(p = 0.81)和焦虑程度(p = 0.81)相似;两组的欧洲五维视觉模拟量表(EQ-VAS)评分相似(p = 0.