Gupta Saksham, Nawabi Noah L, Emani Siva, Medeiros Lila, Bernstock Joshua D, Duvall Julia, Ng Patrick, Smith Timothy R, Wen Patrick Y, Reardon David A, Arnaout Omar
Department of Neurosurgery, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
College of Medicine, Medical University of South Carolina, Charleston, SC, USA.
Neurooncol Adv. 2023 Apr 21;5(1):vdad046. doi: 10.1093/noajnl/vdad046. eCollection 2023 Jan-Dec.
Grade 3 1p/19q co-deleted oligodendroglioma is an uncommon primary CNS tumor with a high rate of progression and recurrence. This study examines the benefit of surgery after progression and identifies predictors of survival.
This is a single-institution retrospective cohort study of consecutive adult patients with anaplastic or grade 3 1p/19q co-deleted oligodendroglioma diagnosed between 2001 and 2020.
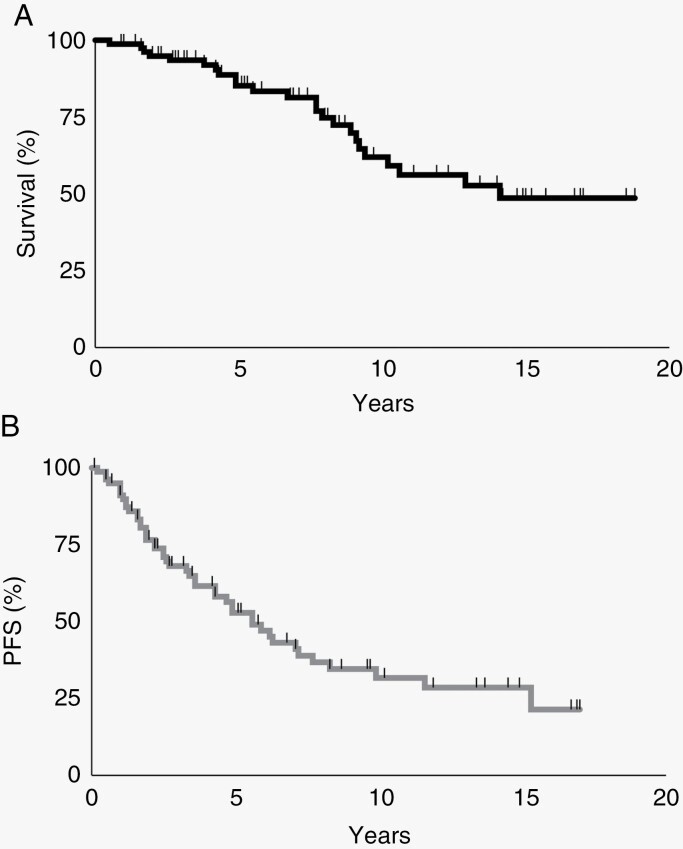
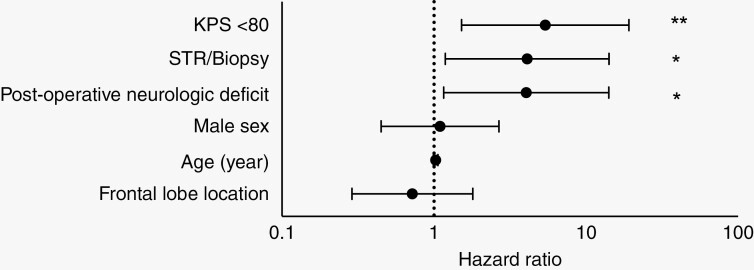
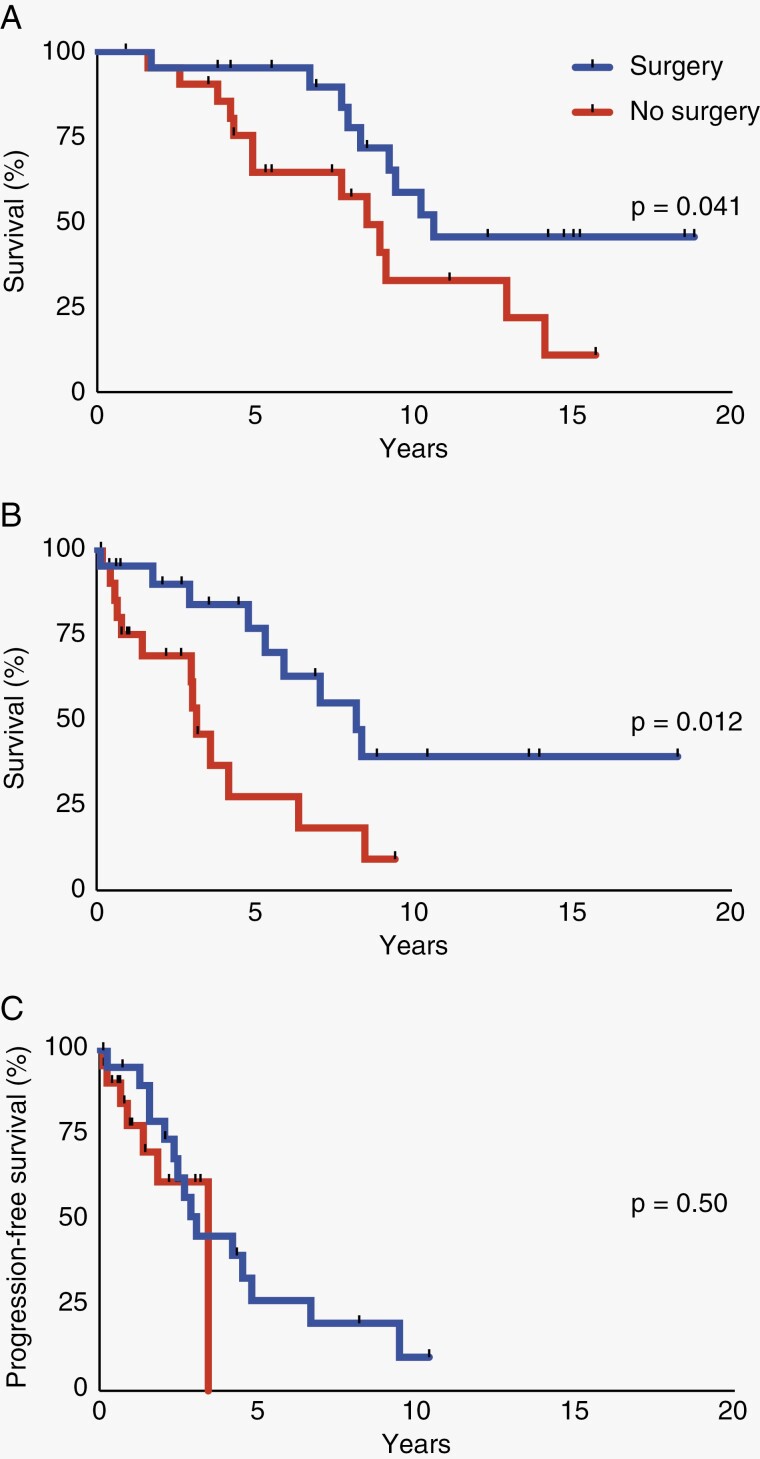
Eighty patients with 1p/19q co-deleted grade 3 oligodendroglioma were included. The median age was 47 years (interquartile range 38-56) and 38.8% were women. All patients underwent surgery, including gross total resection (GTR) for 26.3% of patients, subtotal resection (STR) for 70.0% of patients, and biopsy for 3.8% of patients. Forty-three cases (53.8%) progressed at a median of 5.6 years, and the median overall survival (OS) was 14.1 years. Among 43 cases of progression or recurrence, 21 (48.8%) underwent another resection. Patients who underwent a second operation had improved OS ( = .041) and survival after progression/recurrence ( = .012), but similar time to subsequent progression as patients who did not have repeat surgery ( = .50). Predictors of mortality at initial diagnosis included a preoperative Karnofsky Performance Status (KPS) under 80 (hazard ratio [HR] 5.4; 95% CI 1.5-19.2), an STR or biopsy rather than GTR (HR 4.1; 95% CI 1.2-14.2), and a persistent postoperative neurologic deficit (HR 4.0; 95% CI 1.2-14.1).
Repeat surgery is associated with increased survival, but not time to subsequent progression for progressing or recurrent 1p/19q co-deleted grade 3 oligodendrogliomas recur. Mortality is associated with a preoperative KPS under 80, lack of GTR, and persistent postoperative neurologic deficits after the initial surgery.
3级1p/19q共缺失少突胶质细胞瘤是一种罕见的原发性中枢神经系统肿瘤,进展和复发率高。本研究探讨进展后手术的益处并确定生存预测因素。
这是一项单机构回顾性队列研究,研究对象为2001年至2020年间确诊的连续性成年间变性或3级1p/19q共缺失少突胶质细胞瘤患者。
纳入80例1p/19q共缺失的3级少突胶质细胞瘤患者。中位年龄为47岁(四分位间距38 - 56岁),女性占38.8%。所有患者均接受了手术,其中26.3%的患者接受了全切除(GTR),70.0%的患者接受了次全切除(STR),3.8%的患者接受了活检。43例(53.8%)患者在中位时间5.6年时出现进展,中位总生存期(OS)为14.1年。在43例进展或复发的病例中,21例(48.8%)接受了再次切除。接受二次手术的患者OS改善(P = .041),进展/复发后的生存期改善(P = .012),但与未进行重复手术的患者相比,至后续进展的时间相似(P = .50)。初始诊断时的死亡预测因素包括术前卡氏功能状态(KPS)低于80(风险比[HR] 5.4;95%置信区间1.5 - 19.2)、STR或活检而非GTR(HR 4.1;95%置信区间1.2 - 14.2)以及术后持续存在神经功能缺损(HR 4.0;95%置信区间1.2 - 14.1)。
对于进展或复发的1p/19q共缺失3级少突胶质细胞瘤,重复手术与生存期延长相关,但与至后续进展的时间无关。死亡率与术前KPS低于80、未行GTR以及初次手术后持续存在神经功能缺损有关。