Department of Medicine, University of Mississippi Medical Center, Jackson.
Baylor Scott and White Research Institute, Dallas, Texas.
JAMA Cardiol. 2023 Jul 1;8(7):640-649. doi: 10.1001/jamacardio.2023.1090.
The diuretic effect of sodium-glucose cotransporter 2 inhibitors may result in interaction with background diuretic therapy in patients with heart failure and preserved ejection fraction (HFpEF).
To assess the safety and efficacy of empagliflozin in combination with background diuretic therapy and the association of empagliflozin with the need for conventional diuretics.
DESIGN, SETTING, AND PARTICIPANTS: This was a post hoc analysis of the Empagliflozin Outcome Trial in Patients with Chronic Heart Failure with Preserved Ejection Fraction (EMPEROR-Preserved). EMPEROR-Preserved was a phase 3, randomized, placebo-controlled, double-blind clinical trial conducted from March 2017 to April 2021. Patients with class II to IV heart failure and left ventricular ejection fraction greater than 40% were included. Of 5988 patients enrolled, 5815 (97.1%) had baseline data on diuretic use and were included in this analysis, which was conducted from November 2021 to August 2022.
Participants in EMPEROR-Preserved were randomized to empagliflozin or placebo. In this analysis, participants were divided into 4 subgroups: no diuretics and furosemide-equivalent diuretic dose of less than 40 mg, 40 mg, and greater than 40 mg at baseline.
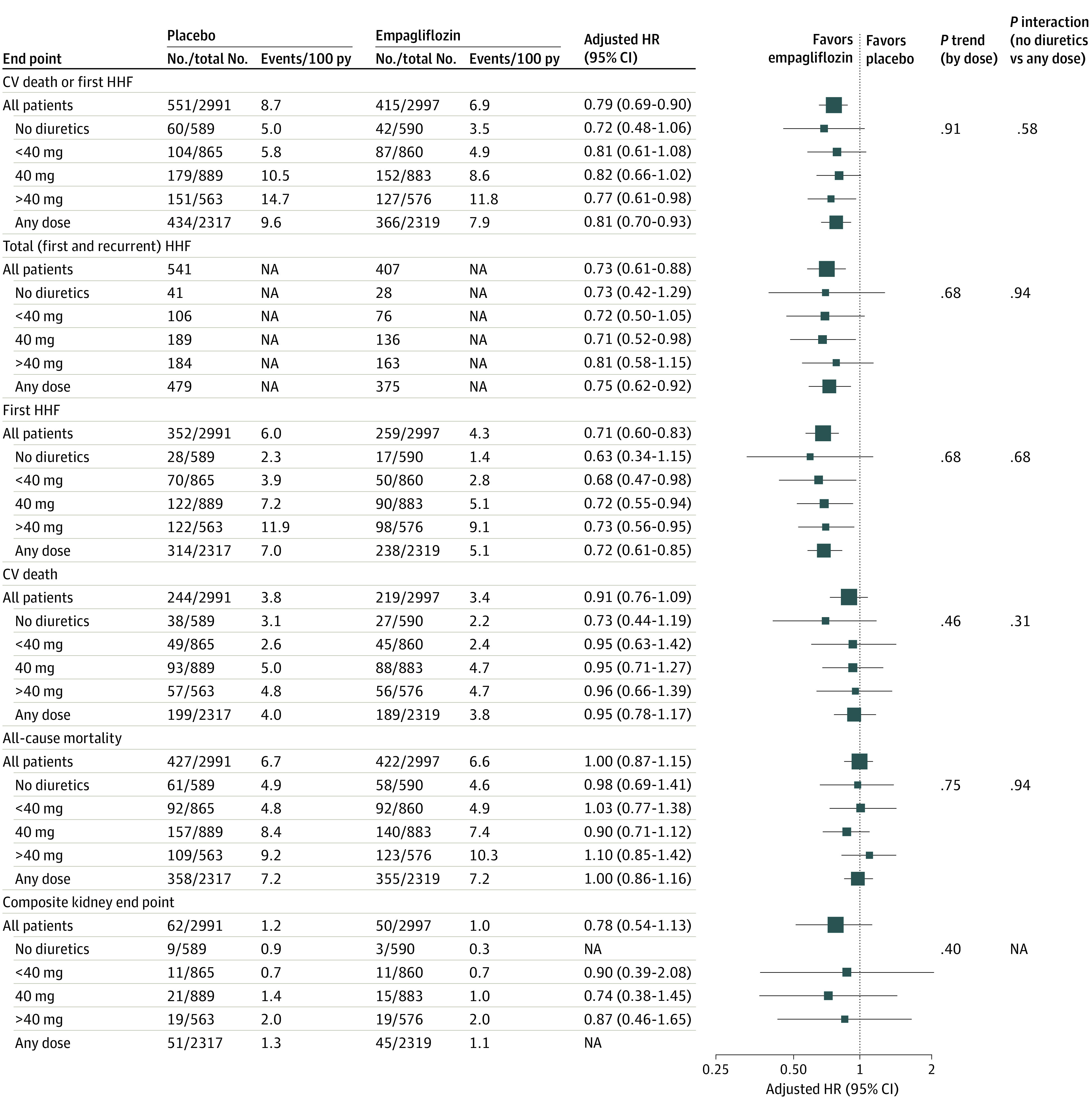
The main outcomes of interest were first hospitalization for heart failure (HHF) or cardiovascular death (CV death) and its components. Association of empagliflozin vs placebo with outcomes by baseline diuretic status (no diuretic vs any dose) and dose (no diuretic, <40 mg, 40 mg, and > 40mg) was assessed. Association of empagliflozin use with changes in diuretic therapy was also studied.
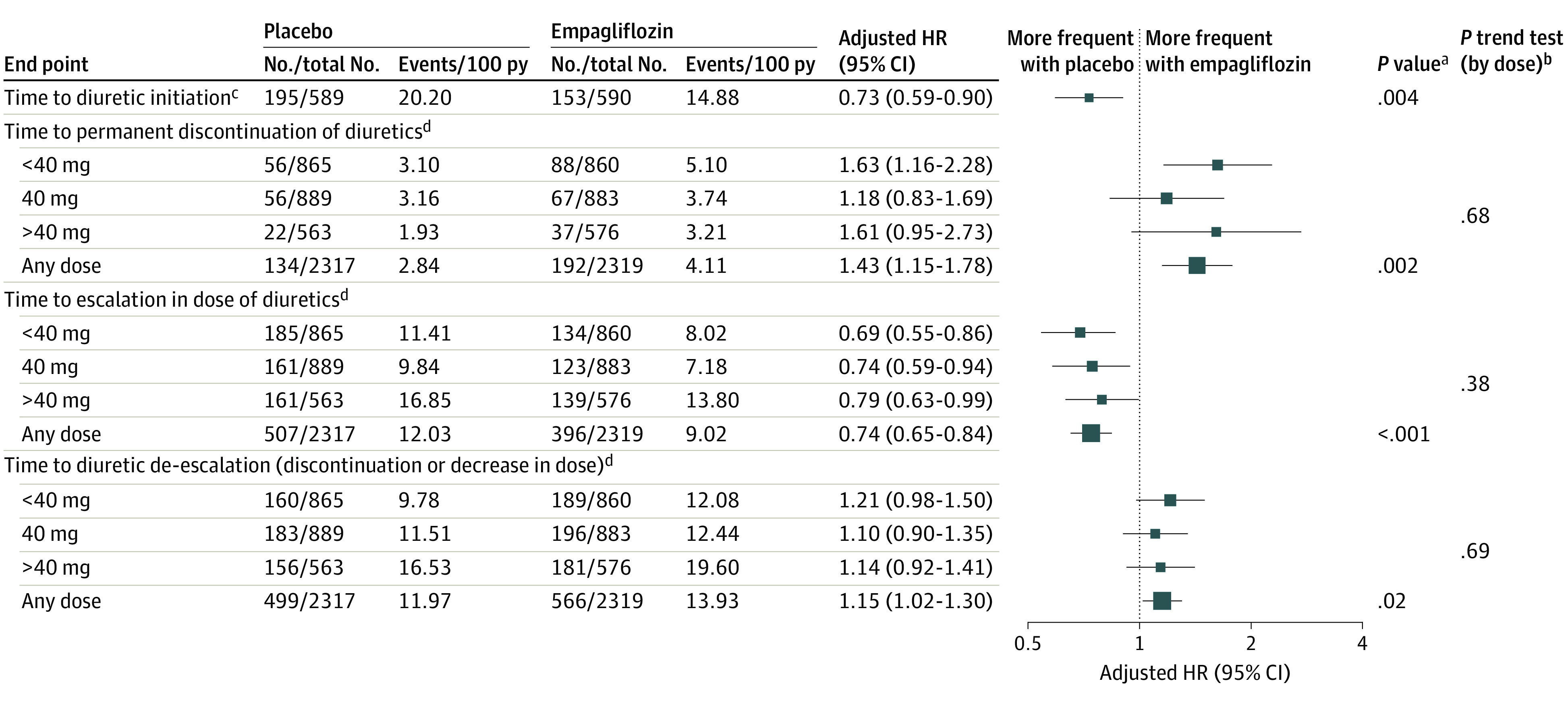
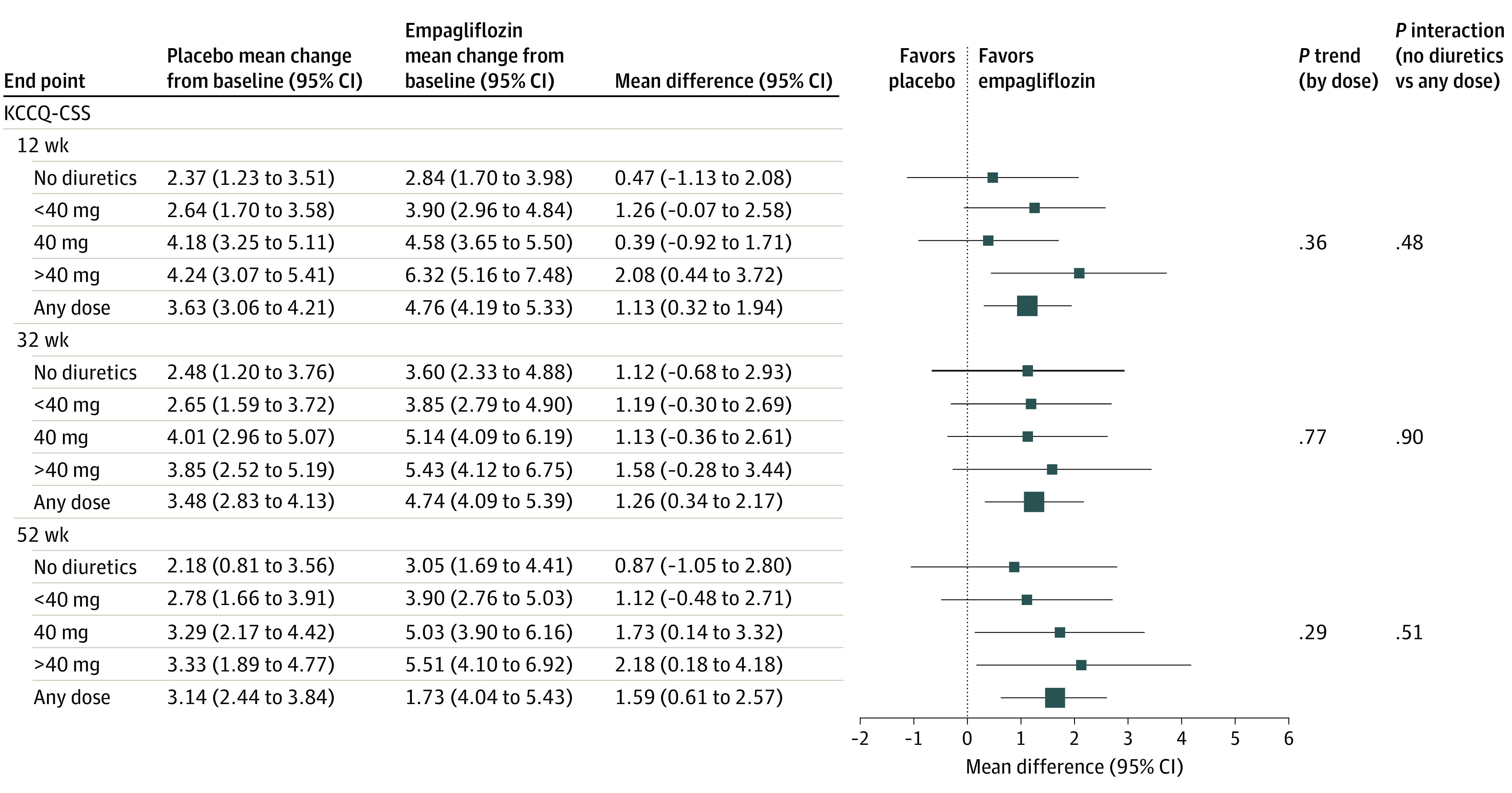
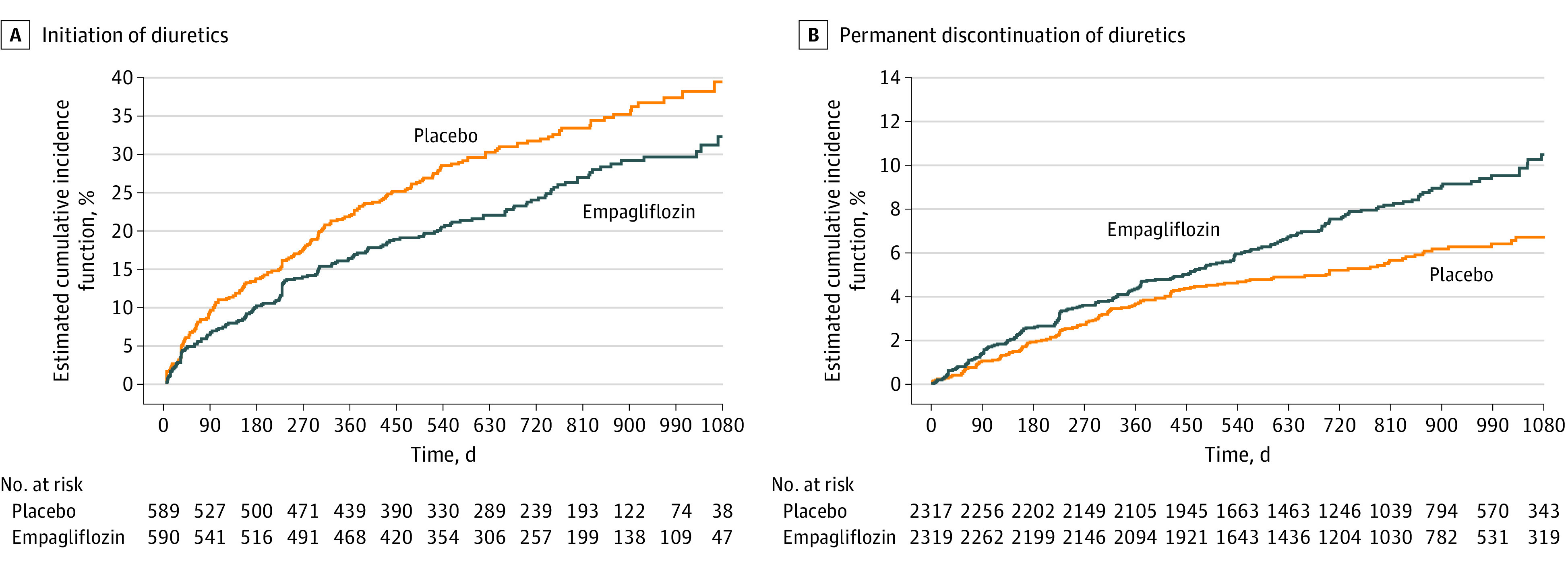
Among 5815 patients (mean [SD] age, 71.9 [9.4] years; 2594 [44.6%] female) with known baseline diuretic use, 1179 (20.3%) were not taking diuretics, 1725 (29.7%) were taking less than 40 mg, 1772 (30.5%) were taking 40 mg, and 1139 (19.6%) were taking greater than 40 mg. In the placebo arm, patients with higher diuretic doses had worse outcomes. Empagliflozin decreased the risk of HHF or CV death, regardless of background diuretic status (hazard ratio [HR], 0.81; 95% CI, 0.70-0.93] for the diuretic group vs HR, 0.72; 95% CI, 0.48-1.06 for the nondiuretic group; P for interaction = .58). Similarly, diuretic status was not associated with changes in improvements in first HHF, total HHF, rate of decline in estimated glomerular filtration rate, and Kansas City Cardiomyopathy Questionnaire 23 clinical summary score with empagliflozin. Findings were consistent when patients were categorized by diuretic dose. Empagliflozin was associated with a decreased likelihood of diuretic dose escalation (HR, 0.74; 95% CI, 0.65-0.84) and an increased likelihood of de-escalation (HR, 1.15; 95% CI, 1.02-1.30). Empagliflozin was associated with an increased risk of volume depletion in patients taking diuretics (HR, 1.34; 95% CI, 1.13-1.59).
In this study, treatment with empagliflozin was similar regardless of diuretic use or dose. Empagliflozin use was associated with decreased conventional diuretic dosing.
ClinicalTrials.gov Identifier: NCT03057951.
钠-葡萄糖协同转运蛋白 2 抑制剂的利尿作用可能导致心力衰竭和射血分数保留(HFpEF)患者与背景利尿剂治疗相互作用。
评估恩格列净联合背景利尿剂治疗的安全性和有效性,以及恩格列净与常规利尿剂需求的关联。
设计、地点和参与者:这是慢性心力衰竭伴射血分数保留的恩格列净结局试验(EMPEROR-Preserved)的事后分析。EMPEROR-Preserved 是一项 III 期、随机、安慰剂对照、双盲临床试验,于 2017 年 3 月至 2021 年 4 月进行。包括 II 级至 IV 级心力衰竭和左心室射血分数大于 40%的患者。在 5988 名入组患者中,有 5815 名(97.1%)基线时使用利尿剂的数据,包括在本次分析中,该分析于 2021 年 11 月至 2022 年 8 月进行。
参与者被随机分配至恩格列净或安慰剂。在本分析中,参与者被分为 4 个亚组:无利尿剂和呋塞米等效剂量小于 40mg、40mg 和大于 40mg。
主要观察终点是首次心力衰竭(HFH)或心血管死亡(CV 死亡)及其组成部分的首次住院。评估恩格列净与安慰剂在基线利尿剂状态(无利尿剂与任何剂量)和剂量(无利尿剂、<40mg、40mg 和>40mg)下与结局的相关性。还研究了恩格列净的使用与利尿剂治疗变化的相关性。
在已知基线利尿剂使用情况的 5815 名患者中(平均[标准差]年龄为 71.9[9.4]岁;2594[44.6%]名女性),1179 名(20.3%)未服用利尿剂,1725 名(29.7%)服用的呋塞米等效剂量小于 40mg,1772 名(30.5%)服用 40mg,1139 名(19.6%)服用的剂量大于 40mg。在安慰剂组中,利尿剂剂量较高的患者预后较差。无论背景利尿剂状态如何,恩格列净均降低了 HFH 或 CV 死亡的风险(利尿剂组的危险比[HR],0.81;95%CI,0.70-0.93 与无利尿剂组的 HR,0.72;95%CI,0.48-1.06;P 组间比较=0.58)。同样,利尿剂状态与恩格列净治疗后首次 HFH、总 HFH、估计肾小球滤过率下降率和堪萨斯城心肌病问卷 23 临床综合评分的改善变化无关。当患者按利尿剂剂量分类时,结果一致。恩格列净与利尿剂剂量升级的可能性降低相关(HR,0.74;95%CI,0.65-0.84),与降级的可能性增加相关(HR,1.15;95%CI,1.02-1.30)。恩格列净与服用利尿剂的患者发生容量耗竭的风险增加相关(HR,1.34;95%CI,1.13-1.59)。
在这项研究中,无论利尿剂的使用或剂量如何,恩格列净的治疗效果相似。恩格列净的使用与常规利尿剂剂量减少相关。
ClinicalTrials.gov 标识符:NCT03057951。