Rasalam Roy, Sindone Andrew, Deed Gary, Audehm Ralph G, Atherton John J
Endocrinology and Diabetes Department, Alfred Health, Melbourne, Victoria, Australia.
Faculty of Medicine, University of Melbourne, Melbourne, Victoria, Australia.
ESC Heart Fail. 2025 Jun;12(3):1544-1557. doi: 10.1002/ehf2.15205. Epub 2025 Jan 23.
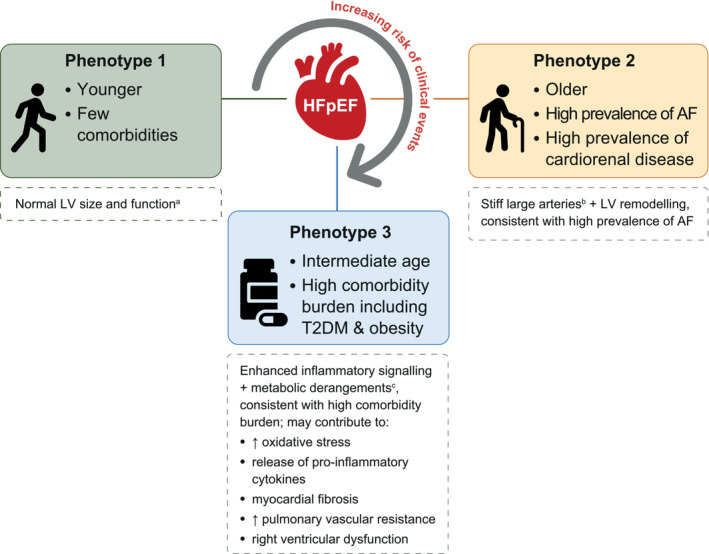
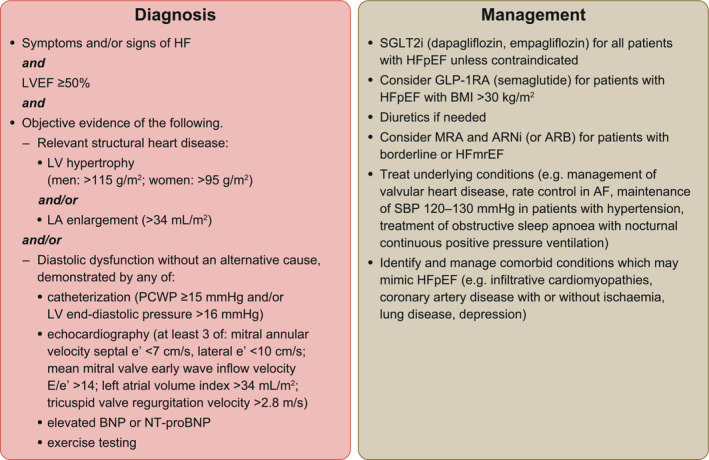
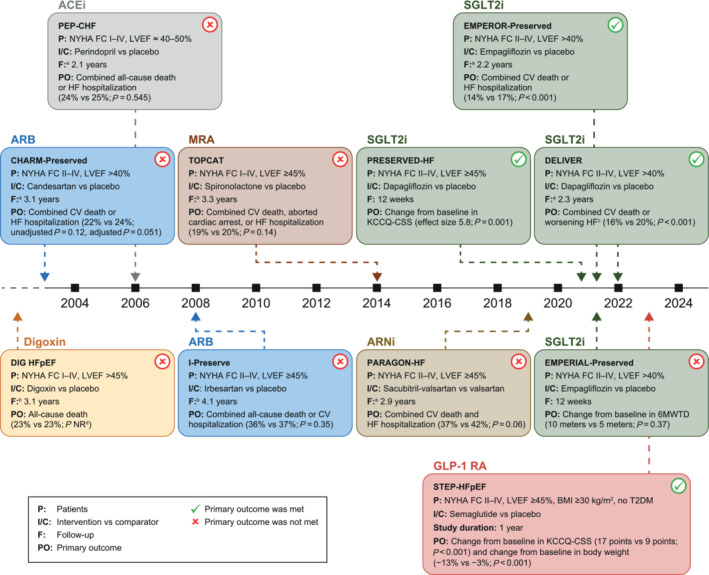
Heart failure with preserved ejection fraction (HFpEF) is defined by heart failure (HF) with a left ventricular ejection fraction (LVEF) of at least 50%. HFpEF has a complex and heterogeneous pathophysiology with multiple co-morbidities contributing to its presentation. Establishing the diagnosis of HFpEF can be challenging. Two algorithms, the 'Heavy, 2 or more Hypertensive drugs, atrial Fibrillation, Pulmonary hypertension, Elderly age >60, elevated Filling pressures' (HFPEF) and the 'Heart Failure Association Pre-test assessment, Echocardiography and natriuretic peptide, Functional testing, Final aetiology' (HFA-PEFF), can help to determine the likelihood of HFpEF in individuals with symptoms of HF. Phenotype clusters defined largely by the total number and types of co-morbidities may delineate groups of patients with HFpEF with different management needs. It is important to recognize alternative diagnoses or HFpEF mimics such as infiltrative cardiomyopathies, coronary artery disease, lung disease, anxiety, depression, anaemia, severe obesity, and physical deconditioning, among others. Treatment with sodium-glucose co-transporter 2 inhibitors (dapagliflozin and empagliflozin) is recommended for all patients with HFpEF unless contraindicated. Future research should consider alternative approaches to guide the initial diagnosis and treatment of HFpEF, including phenotype clustering models and artificial intelligence, and consider whether LVEF is the most useful distinguishing feature for categorizing HF. Ongoing clinical trials are evaluating novel pharmacological and device-based approaches to address the pathophysiological consequences of HFpEF.
射血分数保留的心力衰竭(HFpEF)定义为左心室射血分数(LVEF)至少为50%的心力衰竭(HF)。HFpEF具有复杂且异质性的病理生理学,多种合并症导致其临床表现。确立HFpEF的诊断可能具有挑战性。两种算法,即“重度、2种或更多高血压药物、心房颤动、肺动脉高压、年龄>60岁、充盈压升高”(HFPEF)和“心力衰竭协会预测试评估、超声心动图和利钠肽、功能测试、最终病因”(HFA-PEFF),可帮助确定有HF症状个体患HFpEF的可能性。主要由合并症的总数和类型定义的表型集群可能会划分出具有不同管理需求的HFpEF患者群体。识别诸如浸润性心肌病、冠状动脉疾病、肺部疾病、焦虑、抑郁、贫血、严重肥胖和身体机能减退等替代诊断或HFpEF模拟疾病很重要。除非有禁忌证,推荐对所有HFpEF患者使用钠-葡萄糖协同转运蛋白2抑制剂(达格列净和恩格列净)进行治疗。未来的研究应考虑采用替代方法来指导HFpEF的初始诊断和治疗,包括表型聚类模型和人工智能,并考虑LVEF是否是对HF进行分类最有用的区分特征。正在进行的临床试验正在评估新型药物和基于器械的方法,以解决HFpEF的病理生理后果。