Department of Epidemiology and Health Informatics, Graduate School of Public Health, Korea University, Seoul, Korea.
Department of Internal Medicine, Kangbuk Samsung Medical Center, Seoul, Korea.
PLoS One. 2023 May 25;18(5):e0286246. doi: 10.1371/journal.pone.0286246. eCollection 2023.
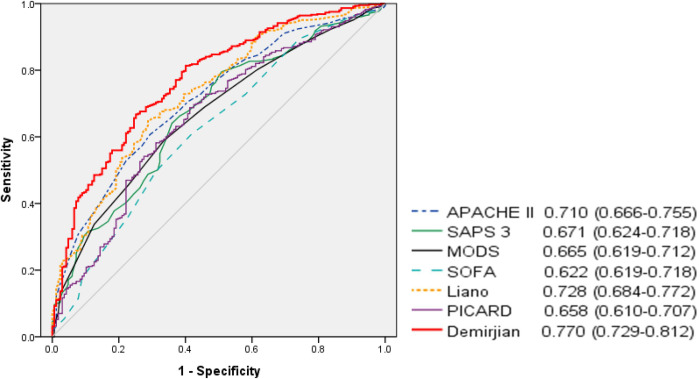
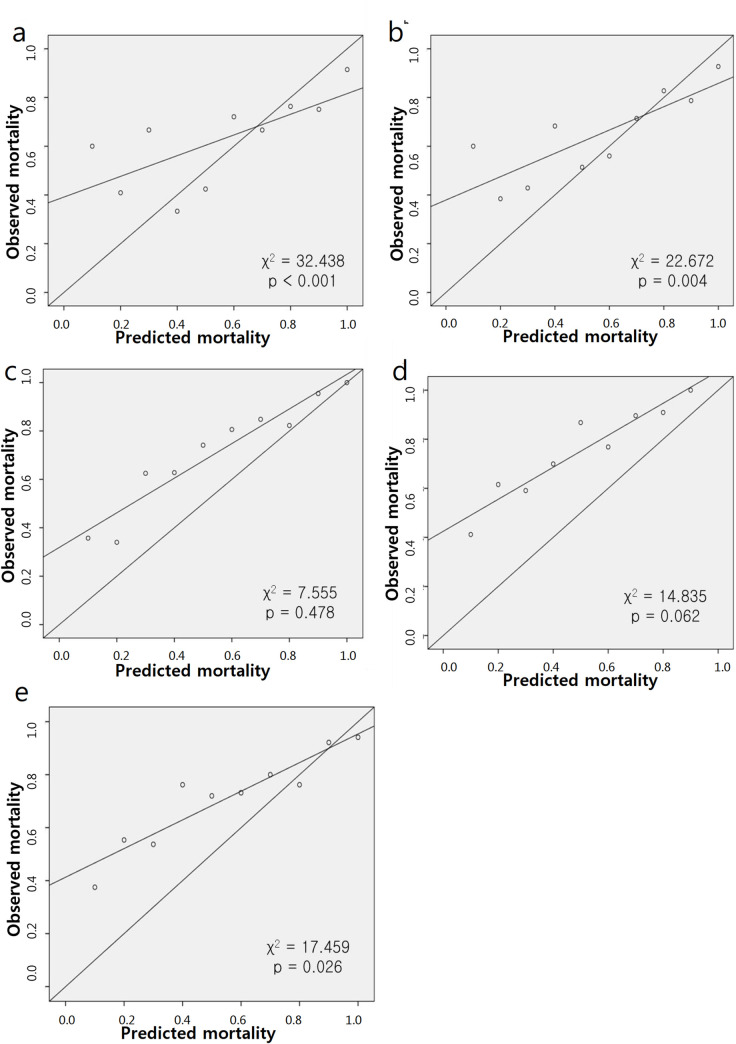
The incidence of acute kidney injury (AKI) is increasing every year and many patients with AKI admitted to the intensive care unit (ICU) require continuous renal replacement therapy (CRRT). This study compared and analyzed severity scoring systems to assess their suitability in predicting mortality in critically ill patients receiving CRRT. Data from 612 patients receiving CRRT in four ICUs of the Korea University Medical Center between January 2016 and November 2018 were retrospectively collected. The mean age of all patients was 67.6 ± 14.8 years, and the proportion of males was 59.6%. The endpoints were in-hospital mortality and 7-day mortality from the day of CRRT initiation to the date of death. The Program to Improve Care in Acute Renal Disease (PICARD), Demirjian's, Acute Physiology and Chronic Health Evaluation (APACHE) II, Simplified Acute Physiology Score (SAPS) 3, Sequential Organ Failure Assessment (SOFA), Multiple Organ Dysfunction Score (MODS), and Liano's scores were used to predict mortality. The in-hospital and 7-day mortality rates in the study population were 72.7% and 45.1%, respectively. The area under the receiver operator characteristic curve (AUROC) revealed the highest discrimination ability for Demirjian's score (0.770), followed by Liano's score (0.728) and APACHE II (0.710). The AUROC curves for the SAPS 3, MODS, and PICARD were 0.671, 0.665, and 0.658, respectively. The AUROC of Demirjian's score was significantly higher than that of the other scores, except for Liano's score. The Hosmer-Lemeshow test on Demirjian's score showed a poor fit in our analysis; however, it was more acceptable than general severity scores. Kidney-specific severity scoring systems showed better performance in predicting mortality in critically ill patients receiving CRRT than general severity scoring systems.
急性肾损伤(AKI)的发病率逐年增加,许多入住重症监护病房(ICU)的 AKI 患者需要连续肾脏替代治疗(CRRT)。本研究比较和分析了严重程度评分系统,以评估其在预测接受 CRRT 的危重症患者死亡率方面的适用性。本研究回顾性收集了 2016 年 1 月至 2018 年 11 月期间在韩国大学医学中心的四个 ICU 接受 CRRT 的 612 例患者的数据。所有患者的平均年龄为 67.6 ± 14.8 岁,男性比例为 59.6%。终点为从 CRRT 开始之日到死亡之日的住院死亡率和 7 天死亡率。用于预测死亡率的评分系统包括:改善急性肾损伤护理计划(PICARD)、德米尔詹(Demirjian)、急性生理学和慢性健康评估(APACHE)Ⅱ、简化急性生理学评分(SAPS)3、序贯器官衰竭评估(SOFA)、多器官功能障碍评分(MODS)和利亚诺(Liano)评分。研究人群的住院死亡率和 7 天死亡率分别为 72.7%和 45.1%。受试者工作特征曲线(ROC)下面积(AUROC)显示德米尔詹(Demirjian)评分具有最高的区分能力(0.770),其次是利亚诺(Liano)评分(0.728)和 APACHE Ⅱ(0.710)。SAPS 3、MODS 和 PICARD 的 AUROC 曲线分别为 0.671、0.665 和 0.658。德米尔詹(Demirjian)评分的 AUROC 明显高于其他评分,除了利亚诺(Liano)评分。德米尔詹(Demirjian)评分的 Hosmer-Lemeshow 检验显示在我们的分析中拟合不良,但比一般严重程度评分更能接受。肾脏特异性严重程度评分系统在预测接受 CRRT 的危重症患者死亡率方面的表现优于一般严重程度评分系统。