Chihota Violet, Gombe Makaita, Gupta Amita, Salazar-Austin Nicole, Ryckman Tess, Hoffmann Christopher J, LaCourse Sylvia, Mathad Jyoti S, Mave Vidya, Dooley Kelly E, Chaisson Richard E, Churchyard Gavin
The Aurum Institute, Parktown, South Africa.
School of Public Health, University of Witwatersrand, Johannesburg, South Africa.
Drugs. 2025 Feb;85(2):127-147. doi: 10.1007/s40265-024-02131-3. Epub 2024 Dec 28.
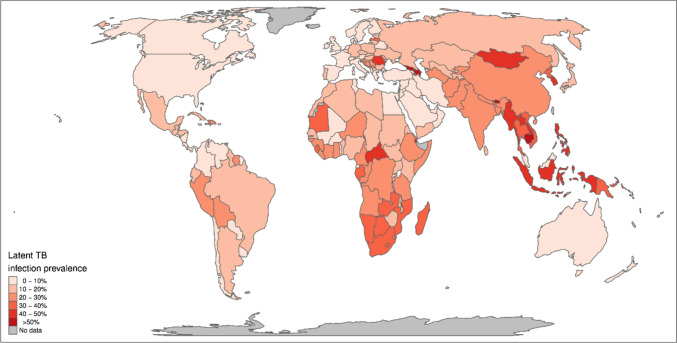
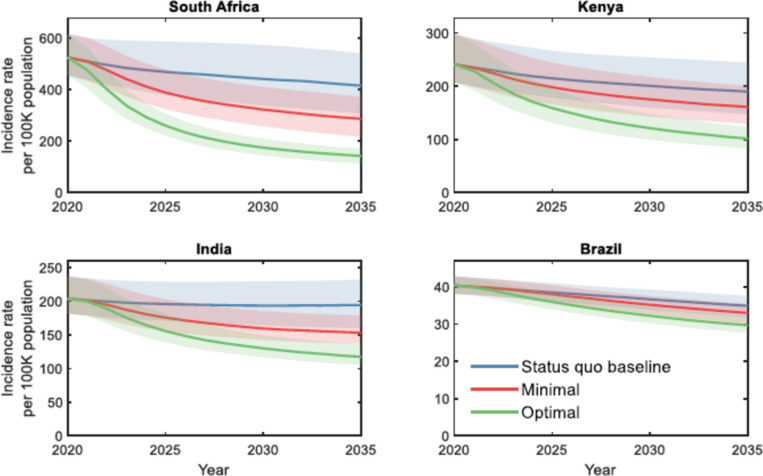
Tuberculosis (TB) is the leading cause of death from a single infectious agent. The burden is highest in some low- and middle-income countries. One-quarter of the world's population is estimated to have been infected with TB, which is the seedbed for progressing from TB infection to the deadly and contagious disease itself. Although some individuals may clear their infections through innate and acquired immunity, many do not. People living with HIV, TB-exposed household contacts, other individuals recently infected, and immunosuppressed individuals are at especially high risk of progressing to TB disease. There have been major advances in recent years to support the programmatic management of TB infection. New tests of infection, including those that predict progression to TB disease, have become available. Numerous World Health Organization-recommended TB preventive treatment (TPT) regimens are available for all ages and for both drug-susceptible and drug-resistant TB infection. All regimens are generally safe, efficacious, and cost effective and have a low risk of generating resistance. TPT is recommended for pregnant women who are at risk for developing TB, but some regimens are associated with an increased likelihood of poor obstetric and fetal outcomes, and newer regimens have not yet been tested in pregnancy. New formulations of rifapentine-based TPT have been developed, and the cost has been radically reduced. Innovative models of delivery to support the scale up of TPT have been developed. Modeling suggests that scaling up TPT, especially regimens with optimal target product profile characteristics, can contribute substantially to ending the TB epidemic. The global uptake of TPT has increased substantially, especially for people living with HIV. Implementation gaps remain, particularly for children, pregnant women, and other household contacts. Further innovation is required to support the continued scale up of TPT and to contribute to ending the TB epidemic.
结核病(TB)是单一传染源导致死亡的首要原因。在一些低收入和中等收入国家,结核病负担最为沉重。据估计,全球四分之一的人口已感染结核菌,而结核菌是从结核感染发展为致命且具传染性疾病的温床。虽然一些个体可通过先天和后天免疫清除感染,但许多人无法做到。感染艾滋病毒者、接触过结核病患者的家庭成员、近期感染的其他个体以及免疫功能低下者进展为结核病的风险尤其高。近年来,在支持结核病感染的规划管理方面取得了重大进展。新的感染检测方法,包括那些可预测进展为结核病的检测方法已问世。世界卫生组织推荐的针对所有年龄段以及药物敏感和耐药结核感染的多种结核病预防性治疗(TPT)方案均已具备。所有方案总体上安全、有效且具有成本效益,产生耐药性的风险较低。对于有患结核病风险的孕妇推荐进行TPT,但一些方案与不良产科和胎儿结局的可能性增加有关,且新方案尚未在孕期进行测试。已研发出基于利福喷丁的TPT新剂型,成本已大幅降低。已开发出支持扩大TPT规模的创新交付模式。模型表明,扩大TPT规模,特别是采用具有最佳目标产品特性的方案,可对终结结核病流行做出重大贡献。全球TPT的使用量大幅增加,尤其是在艾滋病毒感染者中。实施差距依然存在,特别是在儿童、孕妇和其他家庭成员方面。需要进一步创新以支持持续扩大TPT规模并为终结结核病流行做出贡献。