Knott Michael, Hock Stefan, Soder Liam, Mühlen Iris, Kremer Svenja, Sprügel Maximilian I, Sembill Jochen A, Kuramatsu Joji B, Schwab Stefan, Engelhorn Tobias, Doerfler Arnd
Department of Neuroradiology, Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Schwabachanlage 6, 91054 Erlangen, Germany.
Department of Neurology, Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Schwabachanlage 6, 91054 Erlangen, Germany.
J Cardiovasc Dev Dis. 2023 Apr 22;10(5):185. doi: 10.3390/jcdd10050185.
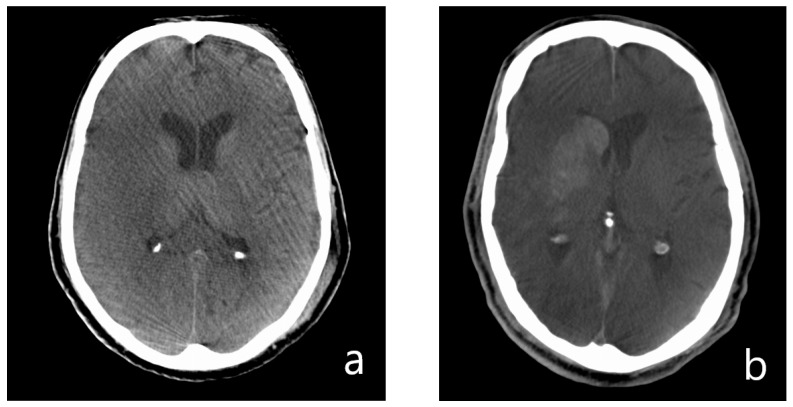
Hyperdense lesions in CT after EVT of LVO are common. These lesions are predictors for haemorrhages and an equivalent of the final infarct. The aim of this study based on FDCT was the evaluation of predisposing factors for these lesions.
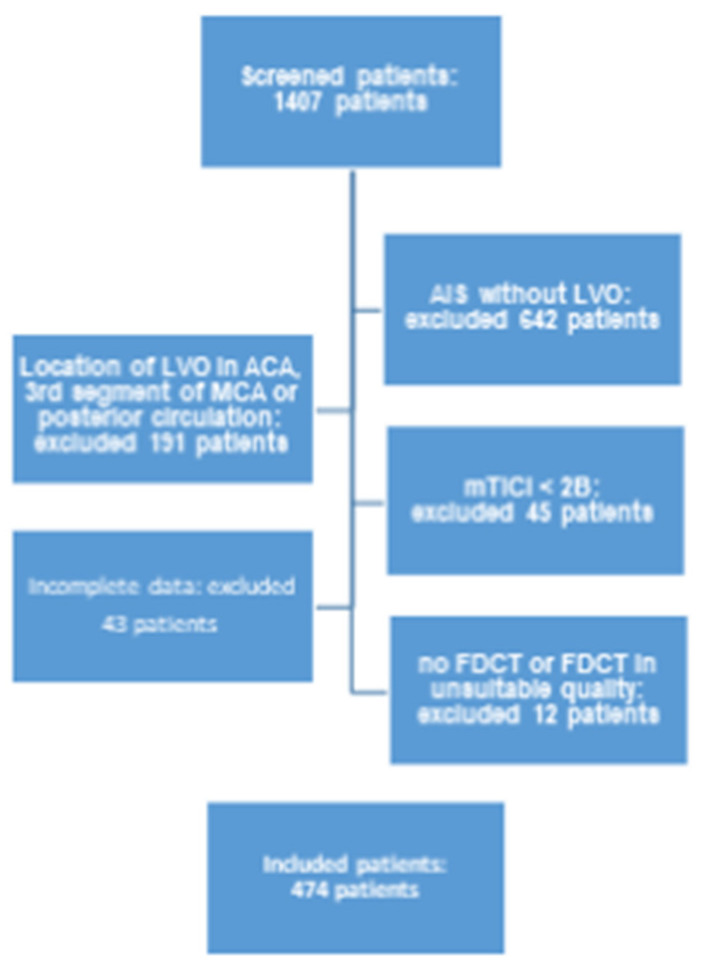
Using a local database, 474 patients with mTICI ≥ 2B after EVT were recruited retrospectively. A postinterventional FDCT after recanalisation was analysed regarding such hyperdense lesions. This was correlated with a variety of items (demographics, past medical history, stroke assessment/treatment and short-/long-term follow-up).
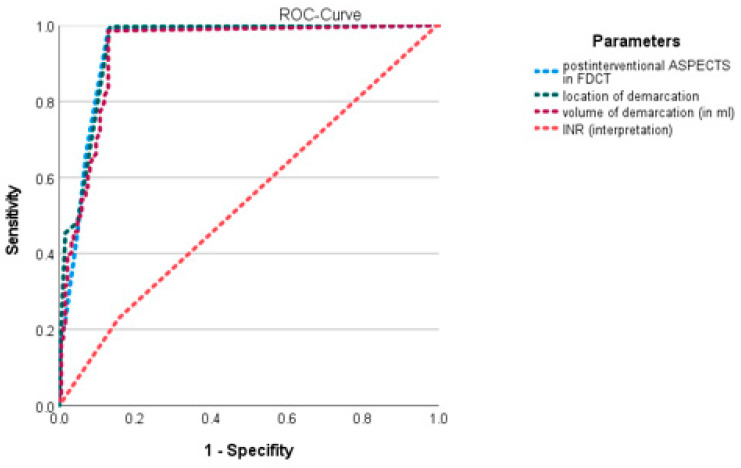
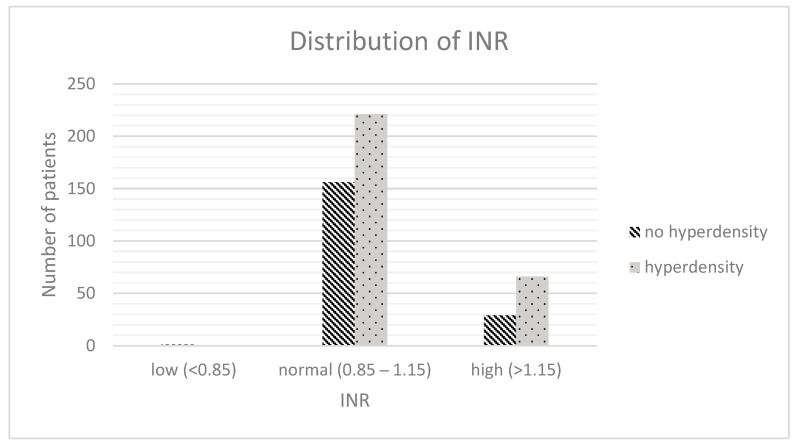
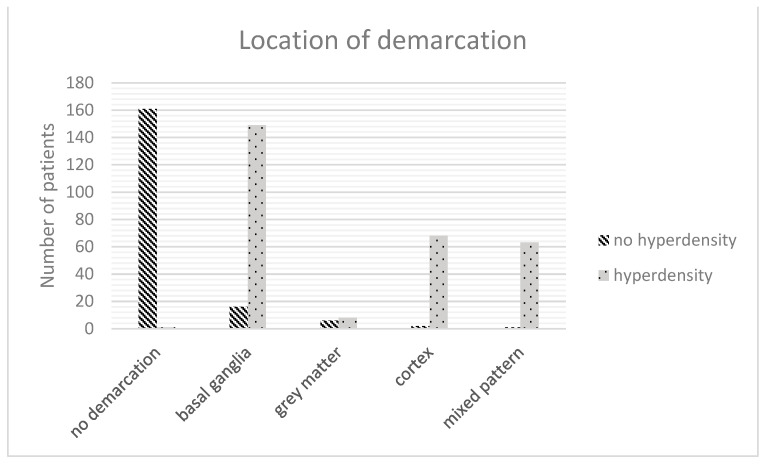
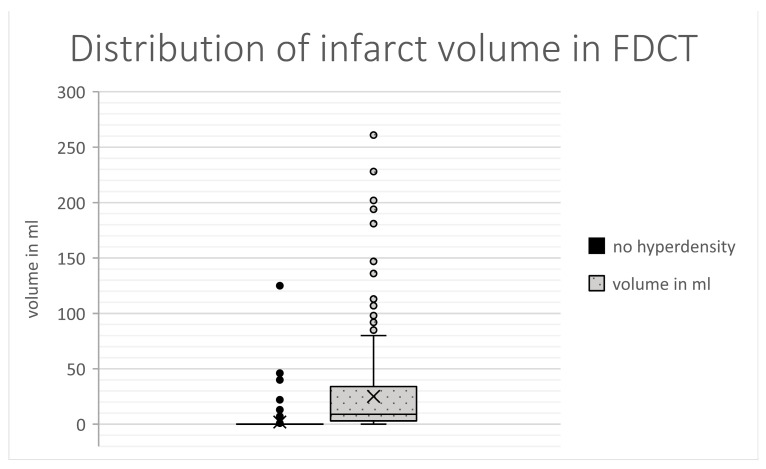
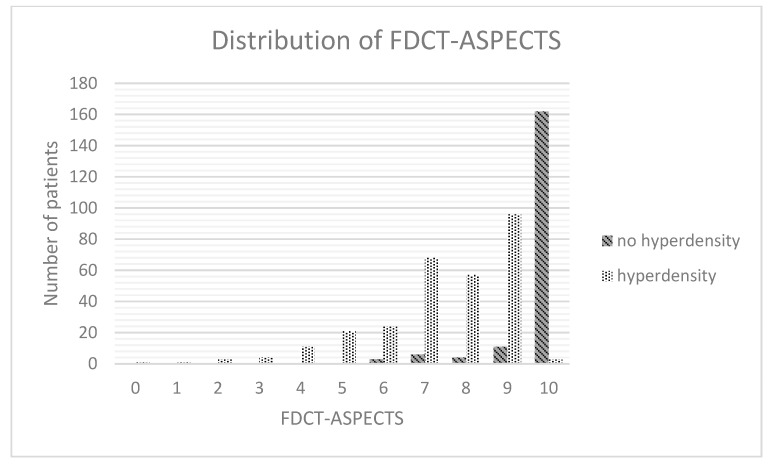
Significant differences were present in NHISS at admission, regarding time window, ASPECTS in initial NECT, location of the LVO, CT-perfusion (penumbra, mismatch ratio), haemostatic parameters (INR, aPTT), duration of EVT, number of EVT attempts, TICI, affected brain region, volume of demarcation and FDCT-ASPECTS. The ICH-rate, the volume of demarcation in follow-up NECT and the mRS at 90 days differed in association with these hyperdensities. INR, the location of demarcation, the volume of demarcation and the FDCT-ASPECTS could be demonstrated as independent factors for the development of such lesions.
Our results support the prognostic value of hyperdense lesions after EVT. We identified the volume of the lesion, the affection of grey matter and the plasmatic coagulation system as independent factors for the development of such lesions.
大血管闭塞(LVO)血管内治疗(EVT)后CT上的高密度病变很常见。这些病变是出血的预测指标,等同于最终梗死灶。本基于双源CT(FDCT)的研究目的是评估这些病变的诱发因素。
利用本地数据库,回顾性纳入474例EVT后改良脑梗死溶栓分级(mTICI)≥2B级的患者。对再通后行介入治疗后的FDCT分析这些高密度病变。将其与各种项目(人口统计学、既往病史、卒中评估/治疗及短期/长期随访)进行关联分析。
在入院时的美国国立卫生研究院卒中量表(NHISS)评分、时间窗、初始非增强CT(NECT)的脑缺血评分(ASPECTS)、LVO的位置、CT灌注(半暗带、不匹配率)、止血参数(国际标准化比值(INR)、活化部分凝血活酶时间(aPTT))、EVT持续时间、EVT尝试次数、mTICI分级、受累脑区、梗死灶体积及FDCT-ASPECTS方面存在显著差异。颅内出血(ICH)发生率、随访NECT中的梗死灶体积及90天时的改良Rankin量表(mRS)评分与这些高密度病变相关。INR、梗死灶位置、梗死灶体积及FDCT-ASPECTS可被证明是这些病变发生的独立因素。
我们的结果支持EVT后高密度病变的预后价值。我们确定病变体积、灰质受累情况及血浆凝血系统是这些病变发生的独立因素。