Division of Medical Oncology and Hematology, Department of Medicine, Princess Margaret Cancer Center, University of Toronto, ON, Canada.
Division of Hematology and Medical Oncology, Department of Medicine, Jordan University Hospital and School of Medicine, The University of Jordan, Amman, Jordan.
JNCI Cancer Spectr. 2023 Jul 3;7(4). doi: 10.1093/jncics/pkad040.
Presence of circulating tumor DNA (ctDNA) is prognostic in solid tumors treated with curative intent. Studies have evaluated ctDNA at specific "landmark" or multiple "surveillance" time points. However, variable results have led to uncertainty about its clinical validity.
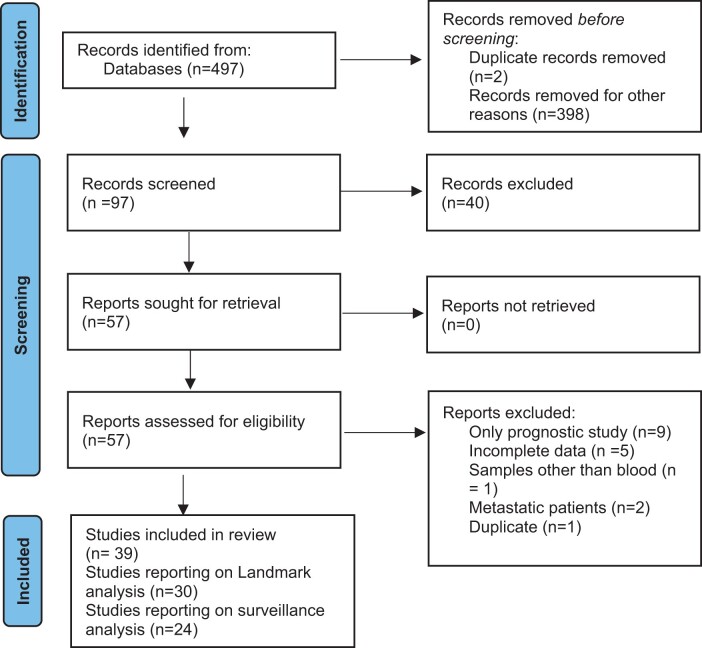
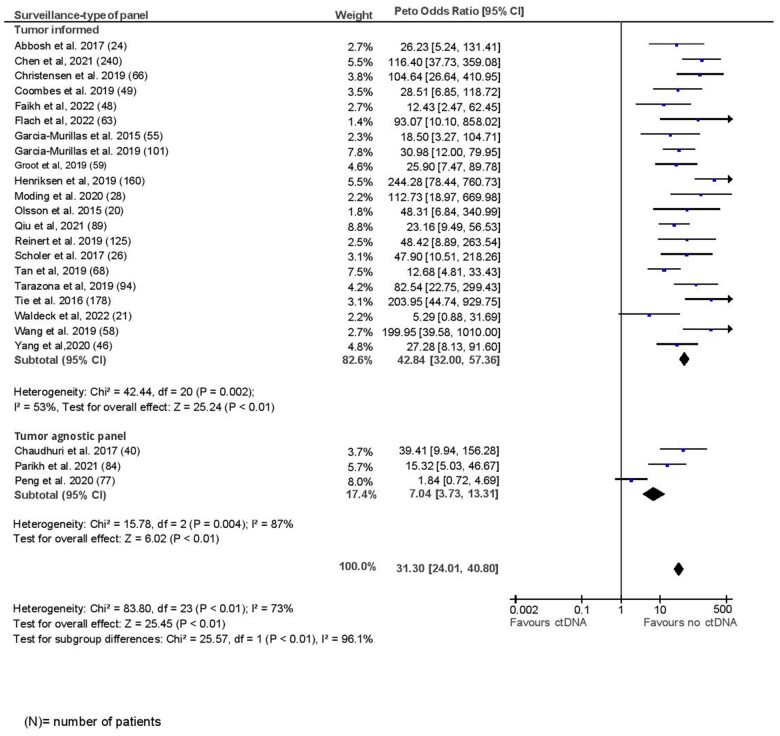
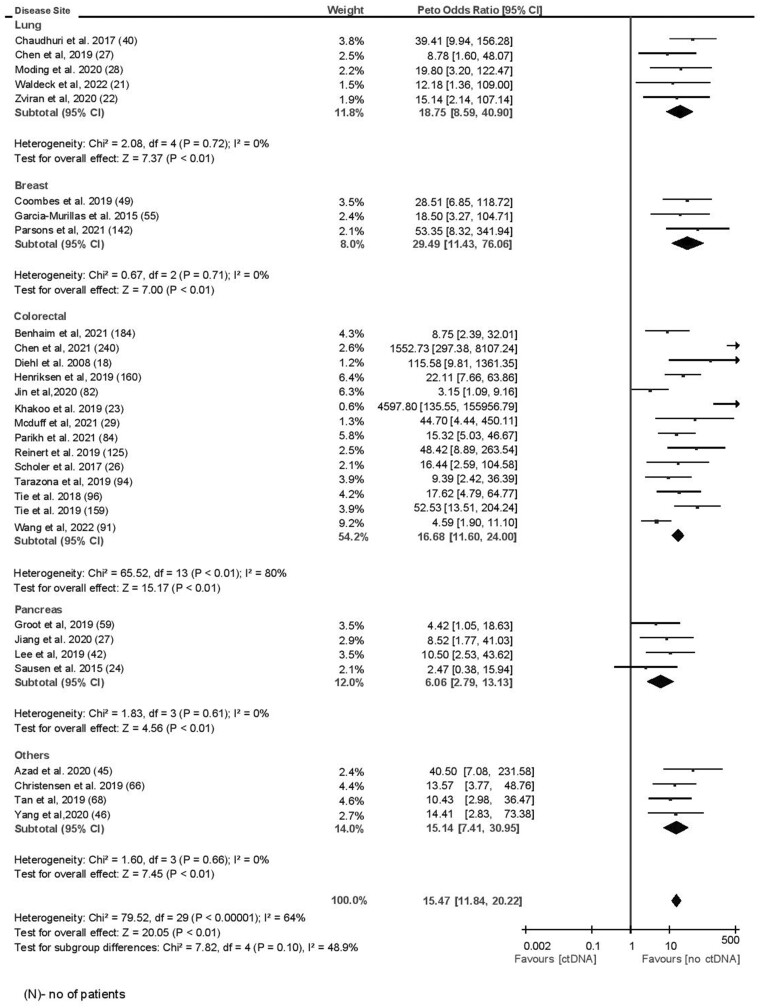
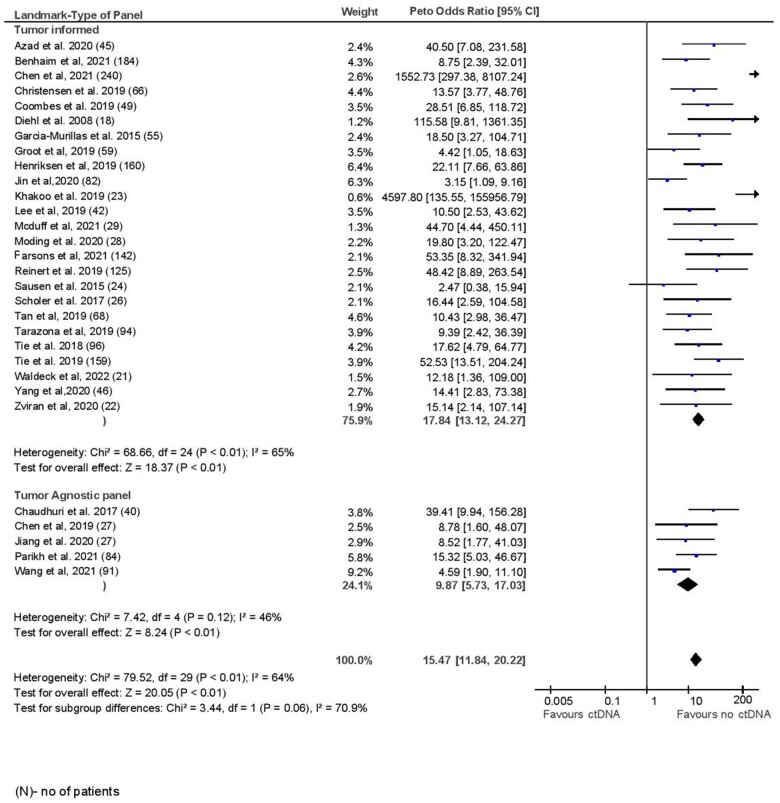
A PubMed search identified relevant studies evaluating ctDNA monitoring in solid tumors after curative intent therapy. Odds ratios for recurrence at both landmark and surveillance time points for each study were calculated and pooled in a meta-analysis using the Peto method. Pooled sensitivity and specificity weighted by individual study inverse variance were estimated and meta-regression using linear regression weighted by inverse variance was performed to explore associations between patient and tumor characteristics and the odds ratio for disease recurrence.
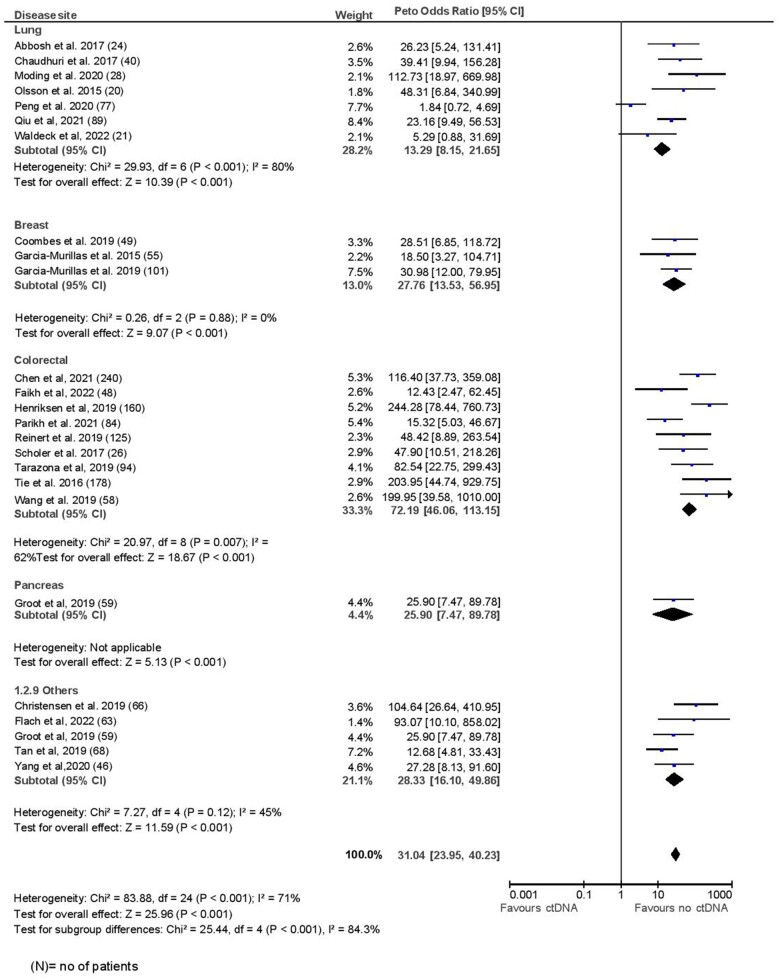
Of 39 studies identified, 30 (1924 patients) and 24 studies (1516 patients) reported on landmark and surveillance time points, respectively. The pooled odds ratio for recurrence at landmark was 15.47 (95% confidence interval = 11.84 to 20.22) and at surveillance was 31.0 (95% confidence interval = 23.9 to 40.2). The pooled sensitivity for ctDNA at landmark and surveillance analyses was 58.3% and 82.2%, respectively. The corresponding specificities were 92% and 94.1%, respectively. Prognostic accuracy was lower with tumor agnostic panels and higher with longer time to landmark analysis, number of surveillance draws, and smoking history. Adjuvant chemotherapy negatively affected landmark specificity.
Although prognostic accuracy of ctDNA is high, it has low sensitivity, borderline high specificity, and therefore modest discriminatory accuracy, especially for landmark analyses. Adequately designed clinical trials with appropriate testing strategies and assay parameters are required to demonstrate clinical utility.
循环肿瘤 DNA(ctDNA)在接受根治性治疗的实体瘤中具有预后价值。研究已经评估了特定“标志性”或多个“监测”时间点的 ctDNA。然而,不同的结果导致其临床有效性存在不确定性。
通过 PubMed 搜索,确定了评估根治性治疗后实体瘤中 ctDNA 监测的相关研究。使用 Peto 法对每个研究的标志性和监测时间点的复发比值比进行计算,并进行荟萃分析。通过个体研究倒数方差加权计算得到的合并敏感性和特异性,并使用倒数方差加权的线性回归进行荟萃回归,以探讨患者和肿瘤特征与疾病复发比值比之间的关系。
在确定的 39 项研究中,30 项(1924 例患者)和 24 项研究(1516 例患者)分别报告了标志性和监测时间点的结果。标志性时间点的复发比值比为 15.47(95%置信区间=11.84 至 20.22),监测时间点为 31.0(95%置信区间=23.9 至 40.2)。ctDNA 对标志性和监测分析的合并敏感性分别为 58.3%和 82.2%,相应的特异性分别为 92%和 94.1%。肿瘤不可知面板的预测准确性较低,而标志性分析时间较长、监测抽提次数较多、有吸烟史的患者的预测准确性较高。辅助化疗对标志性特异性有负面影响。
尽管 ctDNA 的预后准确性较高,但敏感性较低,特异性处于边缘高水平,因此判别准确性适中,尤其是对于标志性分析。需要设计适当的临床试验,采用适当的检测策略和检测参数,以证明其临床应用价值。