Platform of Transfer in Biological Oncology, Georges François Leclerc Cancer Center - UNICANCER, Dijon, France; Genomic and Immunotherapy Medical Institute, Dijon University Hospital, Dijon, France; University of Burgundy-Franche Comté, Maison de l'Université Esplanade Erasme, Dijon, France; UMR INSERM 1231, Dijon, France; Department of Medical Oncology, Georges François Leclerc Cancer Center - UNICANCER, Dijon, France.
Department of Pathology, Besançon University Hospital, Franche-Comté University, Besançon, France; Department of Pathology, Caen University Hospital, Normandy University, Caen, France.
EBioMedicine. 2023 Jun;92:104633. doi: 10.1016/j.ebiom.2023.104633. Epub 2023 May 25.
Anti-PD-1 and PD-L1 antibodies (mAbs) are approved immunotherapy agents to treat metastatic non-small cell lung cancer (NSCLC) patients. Only a minority of patients responds to these treatments and biomarkers predicting response are currently lacking.
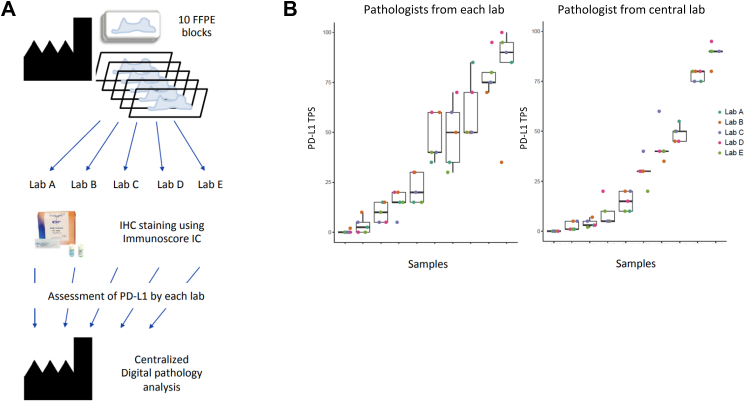
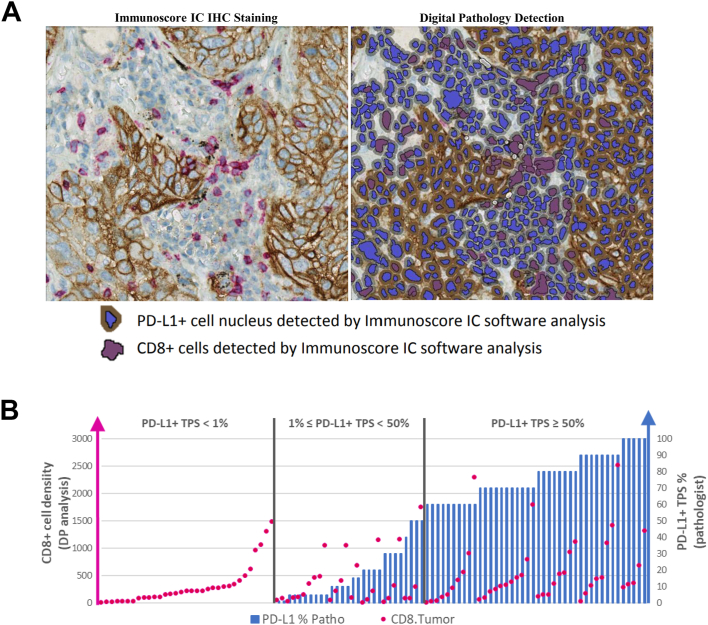
Immunoscore-Immune-Checkpoint (Immunoscore-IC), an in vitro diagnostic test, was used on 471 routine single FFPE-slides, and the duplex-immunohistochemistry CD8 and PD-L1 staining was quantified using digital-pathology. Analytical validation was performed on two independent cohorts of 206 NSCLC patients. Quantitative parameters related to cell location, number, proximity and clustering were analysed. The Immunoscore-IC was applied on a first cohort of metastatic NSCLC patients (n = 133), treated with anti-PD1 or anti-PD-L1 mAbs. Another independent cohort (n = 132) served as validation.
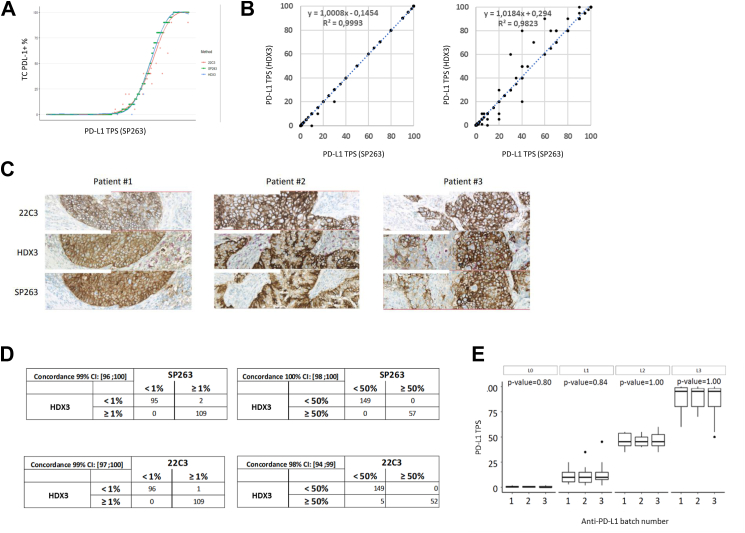
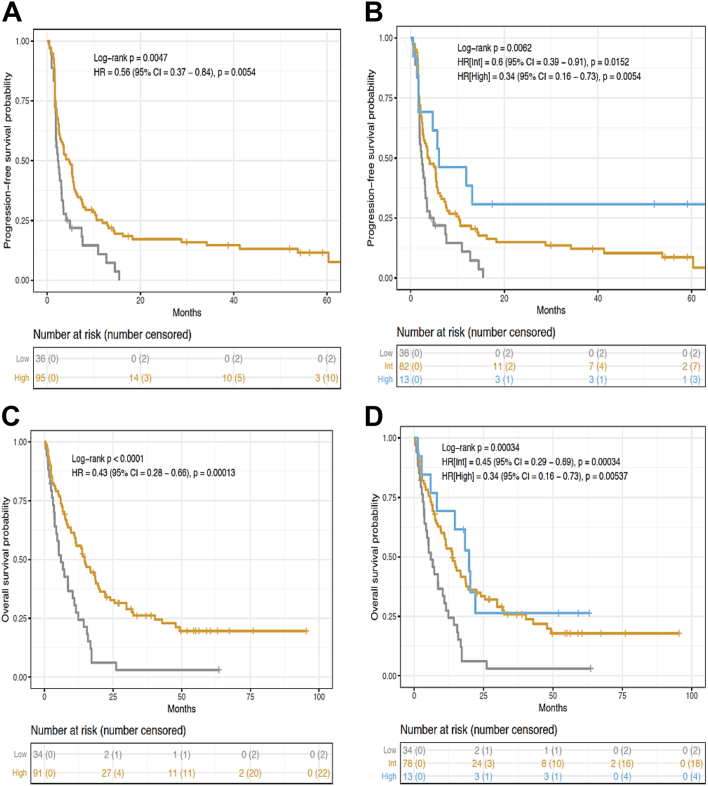
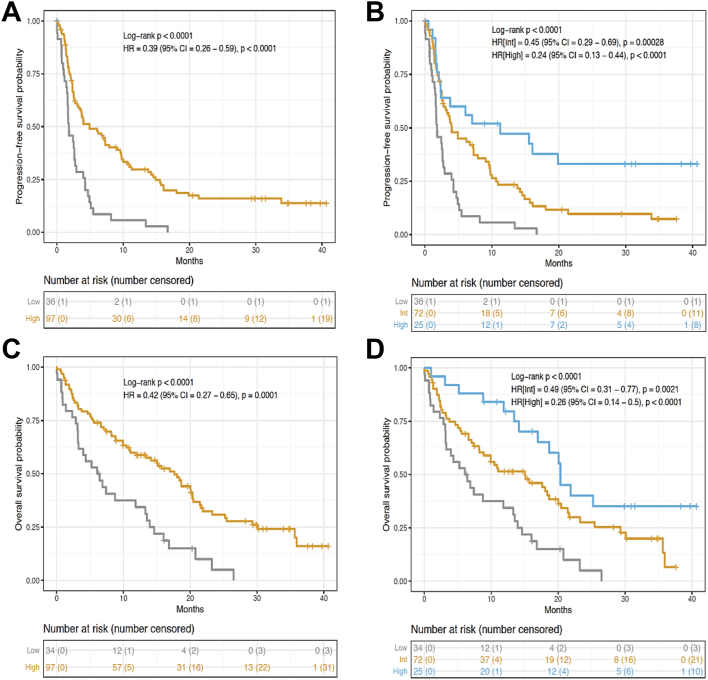
Anti-PDL1 clone (HDX3) has similar characteristics as anti-PD-L1 clones (22C3, SP263). Densities of PD-L1+ cells, CD8+ cells and distances between CD8+ and PD-L1+ cells were quantified and the Immunoscore-IC classification was computed. Using univariate Cox model, 5 histological dichotomised variables (CD8 free of PD-L1+ cells, CD8 clusters, CD8 cells in proximity of PD-L1 cells, CD8 density and PD-L1 cells in proximity of CD8 cells) were significantly associated with Progression-Free Survival (PFS) (all P < 0.0001). Immunoscore-IC classification improved the discriminating power of prognostic model, which included clinical variables and pathologist PD-L1 assessment. In two categories, the Immunoscore-IC risk-score was significantly associated with patients' PFS (HR = 0.39, 95% CI (0.26-0.59), P < 0.0001) and Overall Survival (OS) (HR = 0.42, 95% CI (0.27-0.65), P < 0.0001) in the training-set. Further increased hazard ratios (HR) were found when stratifying patients into three-category Immunoscore-IC (IS-IC). All patients with Low-IS-IC progressed in less than 18 months, whereas PFS at 36 months were 34% and 33% of High-IS-IC patients in the training and validation sets, respectively.
Immunoscore-IC is a powerful tool to predict the efficacy of immune-checkpoint inhibitors (ICIs) in patients with NSCLC.
Veracyte, INSERM, Labex Immuno-Oncology, Transcan ERAnet European project, ARC, SIRIC, CARPEM, Ligue Contre le Cancer, ANR, QNRF, INCa France, Louis Jeantet Prize Foundation.
抗 PD-1 和 PD-L1 抗体(mAb)是已批准的免疫治疗药物,用于治疗转移性非小细胞肺癌(NSCLC)患者。只有少数患者对这些治疗有反应,目前缺乏预测反应的生物标志物。
免疫评分-免疫检查点(Immunoscore-IC)是一种体外诊断测试,在 471 个常规的 FFPE 切片上使用,并用数字病理学对 CD8 和 PD-L1 染色的双重免疫组化进行定量。在 206 名 NSCLC 患者的两个独立队列中进行了分析验证。分析了与细胞位置、数量、接近度和聚类相关的定量参数。将 Immunoscore-IC 应用于接受抗 PD1 或抗 PD-L1 mAb 治疗的转移性 NSCLC 患者的第一个队列(n=133)。另一个独立的队列(n=132)作为验证。
抗 PD-L1 克隆(HDX3)与抗 PD-L1 克隆(22C3、SP263)具有相似的特征。量化了 PD-L1+细胞、CD8+细胞的密度以及 CD8+和 PD-L1+细胞之间的距离,并计算了 Immunoscore-IC 分类。使用单变量 Cox 模型,5 个组织学二分变量(CD8 中无 PD-L1+细胞、CD8 簇、CD8 细胞与 PD-L1 细胞接近、CD8 密度和 PD-L1 细胞与 CD8 细胞接近)与无进展生存期(PFS)显著相关(均 P<0.0001)。免疫评分-IC 分类提高了包括临床变量和病理学家 PD-L1 评估在内的预后模型的区分能力。在两个类别中,免疫评分-IC 风险评分与患者的 PFS(HR=0.39,95%CI(0.26-0.59),P<0.0001)和总生存期(OS)(HR=0.42,95%CI(0.27-0.65),P<0.0001)显著相关。在训练集中,当将患者分层为三分类免疫评分-IC(IS-IC)时,发现进一步增加了危险比(HR)。所有低 IS-IC 患者在 18 个月内均进展,而在训练和验证组中,高 IS-IC 患者的 36 个月 PFS 分别为 34%和 33%。
免疫评分-IC 是预测 NSCLC 患者免疫检查点抑制剂(ICI)疗效的有力工具。
Veracyte、INSERM、Labex 免疫肿瘤学、Transcan ERAnet 欧洲项目、ARC、SIRIC、Carpem、法国癌症协会、法国国家癌症研究所、Louis Jeantet 基金会。