Chebib Fouad T, Zhou Xiaolei, Garbinsky Diana, Davenport Eric, Nunna Sasikiran, Oberdhan Dorothee, Fernandes Ancilla
Division of Nephrology and Hypertension, Mayo Clinic, Jacksonville, FL.
RTI Health Solutions, Research Triangle Park, NC.
Kidney Med. 2023 Apr 14;5(6):100639. doi: 10.1016/j.xkme.2023.100639. eCollection 2023 Jun.
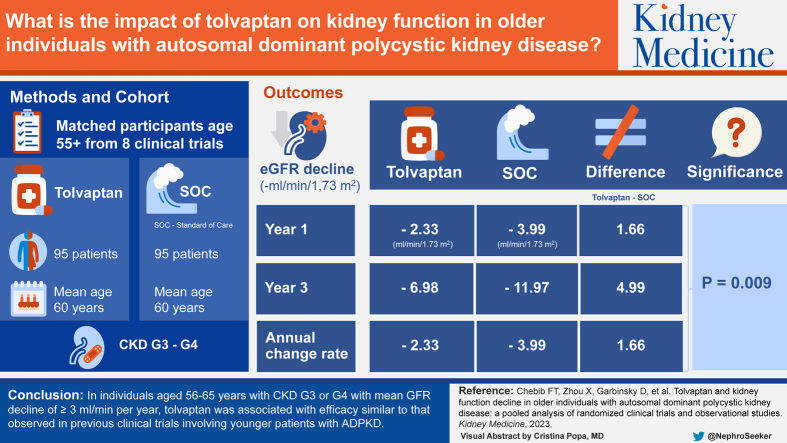
RATIONALE & OBJECTIVE: Tolvaptan is indicated for treatment of patients with autosomal dominant polycystic kidney disease (ADPKD) at risk of rapid progression. Participants aged 56-65 years constituted a small proportion of the Replicating Evidence of Preserved Renal Function: an Investigation of Tolvaptan Safety and Efficacy in ADPKD (REPRISE) trial population. We assessed effects of tolvaptan on estimated glomerular filtration rate (eGFR) decline in participants aged >55 years.
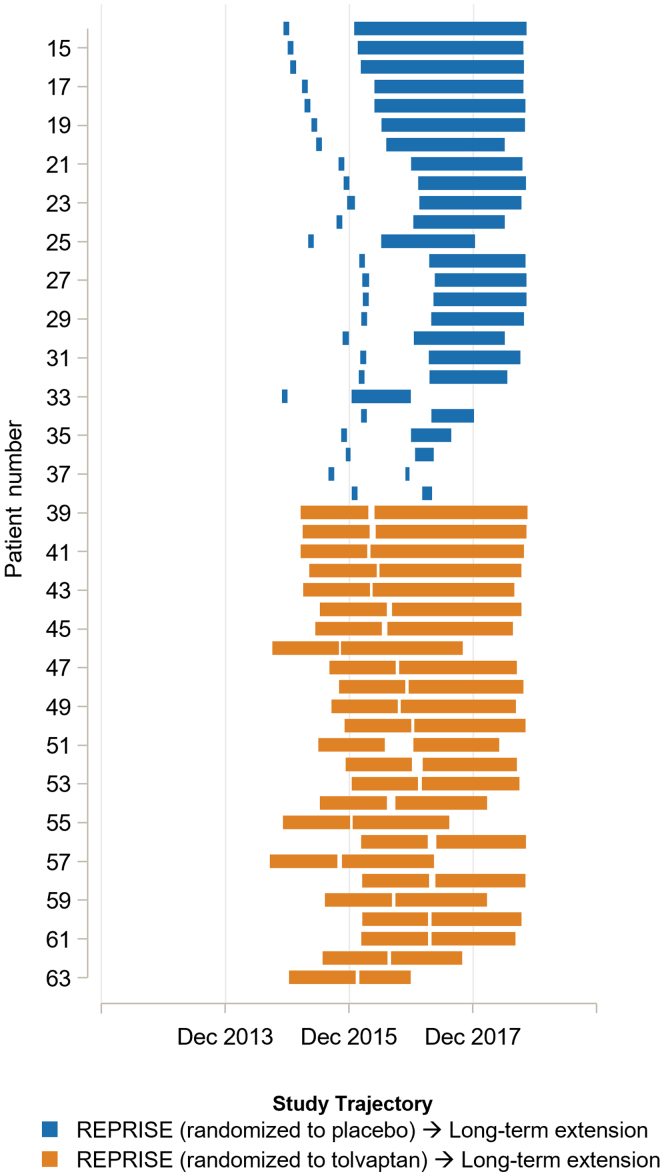
This was a pooled data analysis from 8 studies of tolvaptan or non-tolvaptan standard of care (SOC).
SETTING & PARTICIPANTS: Participants aged >55 years with ADPKD were included. Data on participants in >1 study were linked longitudinally for maximum follow-up duration, with matching for age, sex, eGFR, and chronic kidney disease (CKD) stage to minimize confounding.
Tolvaptan or non-tolvaptan SOC.
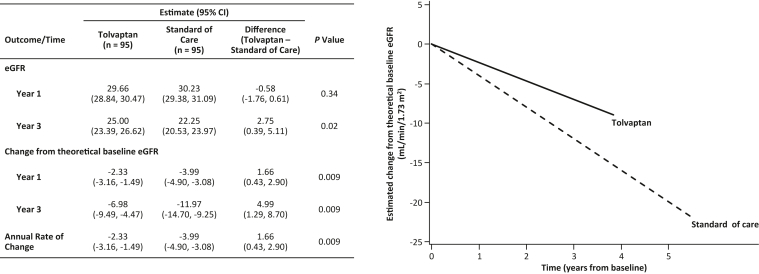
Treatment effects on annualized eGFR decline were compared using mixed models with fixed effects for treatment, time, treatment-by-time interaction, and baseline eGFR.
In the pooled studies, 230 tolvaptan-treated and 907 SOC participants were aged >55 years at baseline. Ninety-five participant pairs from each treatment group were matched, all in CKD G3 or G4, ranging from 56.0 to 65.0 years (tolvaptan) or from 55.1 to 67.0 years (SOC). The eGFR annual decline rate was significantly reduced by 1.66 mL/min/1.73 m (95% CI, 0.43-2.90; = 0.009) in the tolvaptan group compared with SOC (-2.33 versus -3.99 mL/min/1.73 m) over 3 years.
Limitations include potential bias because of study population differences (bias risk was reduced through matching and multiple regression adjustment); vascular disease history data was not uniformly collected, and therefore not adjusted; and natural history of ADPKD precludes evaluating certain clinical endpoints within the study time frame.
In individuals aged 56-65 years with CKD G3 or G4, compared to a SOC group with mean GFR rate of decline ≥3 mL/min/1.73 m/year, tolvaptan was associated with efficacy similar to that observed in the overall indication.
Otsuka Pharmaceutical Development & Commercialization, Inc (Rockville, MD).
TEMPO 2:4 (NCT00413777); phase 1 tolvaptan trial (no NCT number; trial number 156-06-260); phase 2 tolvaptan trial (NCT01336972); TEMPO 4:4 (NCT01214421); REPRISE (NCT02160145); long-term tolvaptan safety extension trial (NCT02251275); OVERTURE (NCT01430494); HALT Progression of Polycystic Kidney Disease (HALT-PKD) study B (NCT01885559).
托伐普坦适用于治疗有快速进展风险的常染色体显性遗传性多囊肾病(ADPKD)患者。年龄在56 - 65岁的参与者在“保留肾功能的重复证据:托伐普坦治疗ADPKD的安全性和有效性研究(REPRISE)”试验人群中占比很小。我们评估了托伐普坦对年龄大于55岁参与者的估计肾小球滤过率(eGFR)下降的影响。
这是一项对8项关于托伐普坦或非托伐普坦标准治疗(SOC)研究的汇总数据分析。
纳入年龄大于55岁的ADPKD患者。对参与1项以上研究的参与者数据进行纵向关联以获得最长随访期,并对年龄、性别、eGFR和慢性肾脏病(CKD)分期进行匹配以尽量减少混杂因素。
托伐普坦或非托伐普坦SOC。
使用包含治疗、时间、治疗与时间交互作用以及基线eGFR固定效应的混合模型比较治疗对年化eGFR下降的影响。
在汇总研究中,230名接受托伐普坦治疗的参与者和907名SOC参与者在基线时年龄大于55岁。每个治疗组匹配了95对参与者,均处于CKD G3或G4期,年龄范围为56.0至65.0岁(托伐普坦组)或55.1至67.0岁(SOC组)。与SOC组相比,托伐普坦组在3年期间eGFR年下降率显著降低1.66 mL/min/1.73m²(95%CI,0.43 - 2.90;P = 0.009)(-2.33对-3.99 mL/min/1.73m²)。
局限性包括由于研究人群差异可能存在的偏倚(通过匹配和多元回归调整降低了偏倚风险);血管疾病史数据收集不统一,因此未进行调整;ADPKD的自然病程使得无法在研究时间框架内评估某些临床终点。
在年龄为56 - 65岁、处于CKD G3或G4期的个体中,与平均GFR下降率≥3 mL/min/1.73m²/年的SOC组相比,托伐普坦的疗效与在总体适应症中观察到的相似。
大冢制药开发与商业化公司(马里兰州罗克维尔)。
TEMPO 2:4(NCT00413777);托伐普坦1期试验(无NCT编号;试验编号156 - 06 - 260);托伐普坦2期试验(NCT01336972);TEMPO 4:4(NCT01214421);REPRISE(NCT02160145);托伐普坦长期安全性扩展试验(NCT02251275);序曲(OVERTURE,NCT01430494);多囊肾病进展停止(HALT - PKD)研究B(NCT01885559)。