Department of Assisted Reproduction, Shanghai Ninth People's Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China.
Center for Reproductive Medicine, Jiangxi Maternal and Child Health Hospital, Nanchang University School of Medicine, Nanchang, China.
BMC Pregnancy Childbirth. 2023 May 30;23(1):401. doi: 10.1186/s12884-023-05596-4.
Previous studies have examined that a range of optimal serum P level during the implantation period was associated with optimal live birth rates. However, those results obtained with vaginal or intramuscular route of progesterone administration for luteal phase support (LPS) alone. Is there a relationship between the serum progesterone (P) on the day of frozen-thawed embryo transfer (FET) with the likelihood of a live birth (LB) in artificial cycles (AC) when using a combination of oral dydrogesterone and vaginal progesterone for LPS?
This was a retrospective study of 3659 FET cycles with artificial endometrial preparation in a Chinese tertiary-care academic medical centre from January 2015 to February 2017. Endometrial preparation was performed using estradiol (E) valerate (Fematon-red tablets) 8 mg/d beginning on day 3 of the cycle, followed by administration of P both orally (8 mg/d Fematon-yellow tablets) and vaginally (400 mg/d; Utrogestan). The primary endpoint was live birth rate (LBR). The association between the serum P level on the embryo transfer day and pregnancy outcomes was evaluated by univariable and multivariable logistic regression analysis.
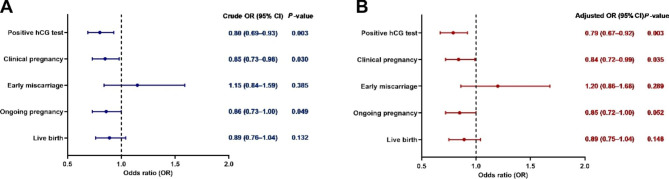
The LBRs according to the serum P quartiles were as follows: Q1: 35.7%; Q2: 37.4%; Q3: 39.1% and Q4: 38.9%. Logistic regression analysis showed that the odds of a LB were not significantly different between the low (P < 7.9 ng/mL) and high (P ≥ 7.9 ng/mL) progesterone groups before or after adjustment (crude OR = 0.89, 95% CI: 0.76-1.04; adjusted OR = 0.89, 95% CI: 0.75-1.04).
The present study suggests that the serum P levels on the day of embryo transfer (ET) do not correlate with the likelihood of a LB in artificial cycles when using a combination of oral dydrogesterone and vaginal progesterone for luteal phase support.
先前的研究已经表明,在胚胎着床期间,一系列最佳的血清 P 水平与最佳活产率有关。然而,这些结果是在单独使用阴道或肌肉途径给予孕激素进行黄体期支持(LPS)时获得的。在使用口服地屈孕酮和阴道孕酮联合进行黄体期支持的人工周期(AC)中,冷冻胚胎移植(FET)日的血清孕激素(P)与活产(LB)的可能性之间是否存在关系?
这是一项在中国一家三级医疗学术中心进行的回顾性研究,纳入了 2015 年 1 月至 2017 年 2 月期间的 3659 个 FET 周期。子宫内膜准备采用戊酸雌二醇(Fematon-red 片剂)8mg/d,从周期第 3 天开始,随后口服(8mg/d Fematon-yellow 片剂)和阴道(400mg/d;Utrogestan)给予 P。主要终点是活产率(LBR)。通过单变量和多变量逻辑回归分析评估 FET 日血清 P 水平与妊娠结局之间的关系。
根据血清 P 四分位数,LBR 如下:Q1:35.7%;Q2:37.4%;Q3:39.1%;Q4:38.9%。逻辑回归分析显示,在未调整或调整后,低(P<7.9ng/ml)和高(P≥7.9ng/ml)孕激素组之间的 LB 几率没有显著差异(粗 OR=0.89,95%CI:0.76-1.04;调整后 OR=0.89,95%CI:0.75-1.04)。
本研究表明,在使用口服地屈孕酮和阴道孕酮联合进行黄体期支持的人工周期中,FET 日的血清 P 水平与 LB 的可能性无关。