IRCCS Ospedale Policlinico San Martino, Largo Benzi 10, 16132, Genoa, Italy.
Pathology Unit, Department of Surgical Sciences and Integrated Diagnostics (DISC), University of Genoa, Genoa, Italy.
Histochem Cell Biol. 2023 Aug;160(2):113-125. doi: 10.1007/s00418-023-02202-8. Epub 2023 Jun 7.
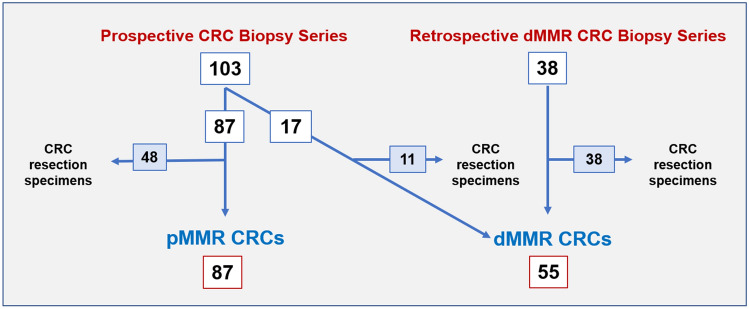
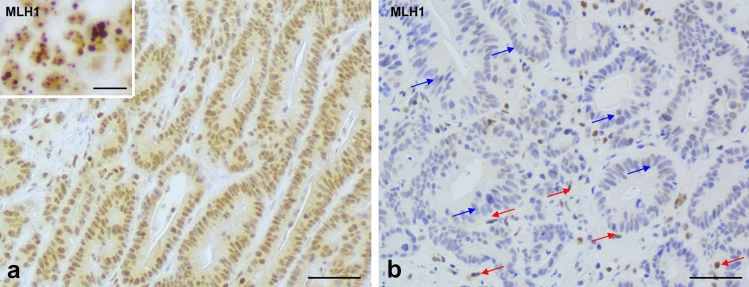
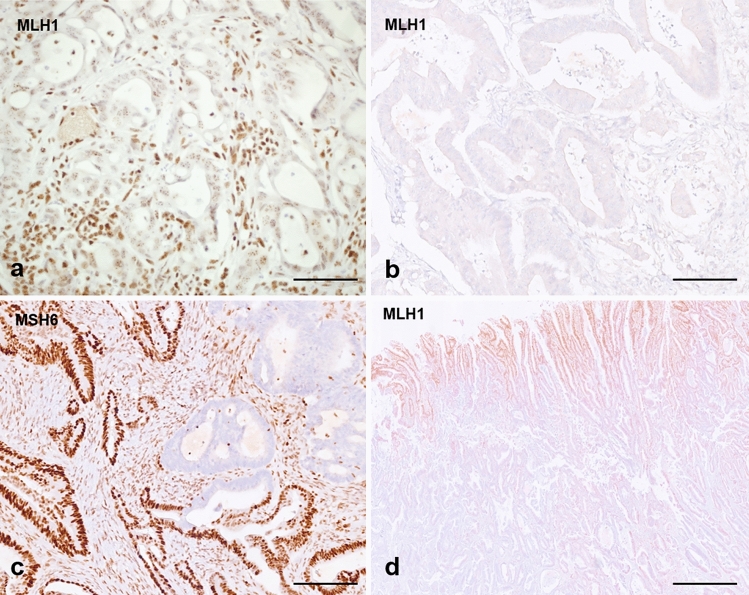
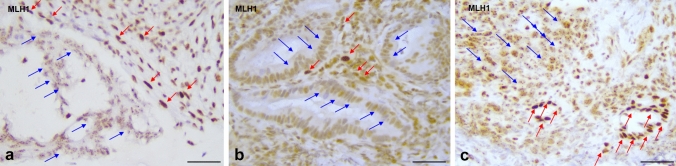
Mismatch repair (MMR) testing on all new cases of colorectal cancer (CRC) has customarily been preferably performed on surgical specimens, as more tissue is available; however, new clinical trials for the use of immune checkpoint inhibitors in the neoadjuvant setting require MMR testing on biopsy samples. This study aims at identifying advantages, disadvantages and any potential pitfalls in MMR evaluation on biopsy tissue and how to cope with them. The study is prospective-retrospective, recruiting 141 biopsies (86 proficient (p)MMR and 55 deficient (d)MMR) and 97 paired surgical specimens (48 pMMR; 49 dMMR). In biopsy specimens, a high number of indeterminate stains was observed, in particular for MLH1 (31 cases, 56.4%). The main reasons were a punctate nuclear expression of MLH1, relatively weak MLH1 nuclear expression compared to internal controls, or both (making MLH1 loss difficult to interpret), which was solved by reducing primary incubation times for MLH1. A mean of ≥ 5 biopsies had adequate immunostains, compared to ≤ 3 biopsies in inadequate cases. Conversely, surgical specimens rarely suffered from indeterminate reactions, while weaker staining intensity (p < 0.007) for MLH1 and PMS2 and increased patchiness grade (p < 0.0001) were seen. Central artefacts were almost exclusive to surgical specimens. MMR status classification was possible in 92/97 matched biopsy/resection specimen cases, and all of these were concordant (47 pMMR and 45 dMMR). Evaluation of MMR status on CRC biopsy samples is feasible, if pitfalls in interpretation are known, making laboratory-specific appropriate staining protocols fundamental for high-quality diagnoses.
错配修复(MMR)检测通常首选在手术标本上进行,因为手术标本中可获得更多的组织;然而,新的临床试验需要在新辅助治疗中使用免疫检查点抑制剂,这就需要对活检样本进行 MMR 检测。本研究旨在确定在活检组织上进行 MMR 评估的优缺点以及任何潜在的陷阱,并探讨如何应对这些问题。本研究为前瞻性回顾性研究,共纳入 141 例活检标本(86 例 MMR 完全(p)和 55 例 MMR 缺失(d))和 97 例配对的手术标本(48 例 pMMR;49 例 dMMR)。在活检标本中,观察到大量不确定的染色,尤其是 MLH1(31 例,56.4%)。主要原因是 MLH1 的点状核表达、与内部对照相比 MLH1 的核表达相对较弱,或者两者兼而有之(使 MLH1 缺失难以解释),通过减少 MLH1 的孵育时间解决了这个问题。与不足 3 例的病例相比,有足够免疫染色的病例平均有≥5 例活检标本,而不足 3 例的病例则有更多的不确定反应。相反,手术标本很少出现不确定的反应,而 MLH1 和 PMS2 的染色强度较弱(p<0.007)和染色不均匀程度增加(p<0.0001)。中心伪影几乎仅见于手术标本。在 97 例匹配的活检/切除标本中,有 92 例能够进行 MMR 状态分类,且所有标本均一致(47 例 pMMR 和 45 例 dMMR)。如果了解解释中的陷阱,对 CRC 活检样本进行 MMR 状态评估是可行的,因此制定针对实验室的具体、高质量诊断的适当染色方案至关重要。