Department of Hematology Oncology, Simon Williamson Clinic, Birmingham, AL, USA.
Alliance Statistics and Data Management Center, Mayo Clinic, Rochester, MN, USA.
Oncologist. 2023 Aug 3;28(8):722-729. doi: 10.1093/oncolo/oyad140.
A protocol was developed to evaluate the value of an NK-1 receptor antagonist for preventing nausea and vomiting resulting from highly emetogenic chemotherapy when an olanzapine-based antiemetogenic regimen was used.
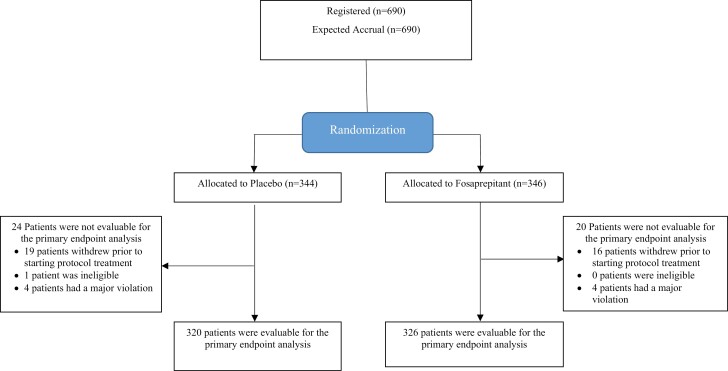
A221602, a prospective double-blind, placebo-controlled clinical trial, was developed to compare 2 -olanzapine-containing antiemetic regimens, one with an NK-1 receptor antagonist (aprepitant or fosaprepitant) and one without. Trial patients had a malignant disease for which they received intravenous highly emetogenic chemotherapy (single day cisplatin ≥ 70 mg/m2 or doxorubicin plus cyclophosphamide on 1 day). Patients on both arms received commonly administered doses of a 5-HT3 receptor antagonist, dexamethasone, and olanzapine. Additionally, patients were randomized to receive an NK-1 receptor antagonist (fosaprepitant 150 mg IV or aprepitant 130 mg IV) or a corresponding placebo. The primary objective was to compare the proportion of patients with no nausea for 5 days following chemotherapy between the 2 study arms. This trial was designed to test for the noninferiority of deleting the NK-1 receptor antagonist, with noninferiority defined as a decrease in freedom from nausea by less than 10%.
A total of 690 patients were entered on this trial, 50% on each arm. The proportion of patients without nausea for the complete 5-day study period was 7.4% lower (upper limit of the one-sided 95% confidence interval was 13.5%) in the arm without an NK-1 receptor antagonist compared with the arm with an NK-1 receptor antagonist.
This trial did not provide sufficient evidence to support that deletion of the NK-1 receptor antagonist was as good as keeping it, as a part of a 4-drug antiemetic regimen for highly emetogenic chemotherapy (ClinicalTrials.gov Identifier: NCT03578081).
制定了一项方案,旨在评估神经激肽-1 受体拮抗剂在使用奥氮平为基础的止吐方案时预防高度致吐性化疗引起的恶心和呕吐的价值。
进行了一项前瞻性、双盲、安慰剂对照的 A221602 临床试验,以比较两种含有奥氮平的止吐方案,一种方案含有神经激肽-1 受体拮抗剂(阿瑞匹坦或福沙匹坦),另一种方案不含神经激肽-1 受体拮抗剂。试验患者患有恶性疾病,接受静脉内高度致吐性化疗(顺铂单天剂量≥70mg/m2 或多柔比星联合环磷酰胺单天剂量)。两组患者均接受了常用剂量的 5-HT3 受体拮抗剂、地塞米松和奥氮平。此外,患者随机接受神经激肽-1 受体拮抗剂(福沙匹坦 150mg 静脉注射或阿瑞匹坦 130mg 静脉注射)或相应的安慰剂。主要目标是比较化疗后 5 天内两组患者无恶心的比例。本试验旨在测试删除神经激肽-1 受体拮抗剂的非劣效性,非劣效性定义为无恶心的比例降低不超过 10%。
共有 690 例患者入组本试验,每组各 50%。在无神经激肽-1 受体拮抗剂组,无恶心的患者比例较有神经激肽-1 受体拮抗剂组低 7.4%(单侧 95%置信区间上限为 13.5%)。
本试验未提供充分证据支持删除神经激肽-1 受体拮抗剂与保留该拮抗剂一样好,作为高度致吐性化疗的 4 药止吐方案的一部分(ClinicalTrials.gov 标识符:NCT03578081)。