Department of Medical Radiation Sciences, Institute of Clinical Sciences, Sahlgrenska Academy, Gothenburg, Sweden;
Department of Oncology, Institute of Clinical Sciences, Sahlgrenska Academy, Gothenburg, Sweden.
J Nucl Med. 2023 Sep;64(9):1456-1462. doi: 10.2967/jnumed.123.265484. Epub 2023 Jun 8.
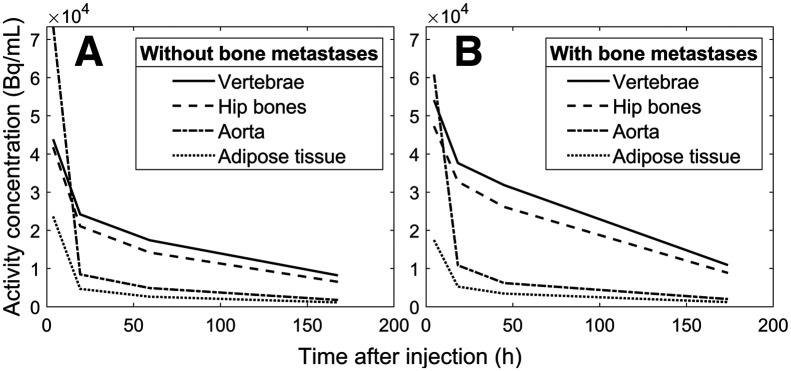
Bone marrow suppression is a common side effect after [Lu]Lu-DOTATATE treatment of neuroendocrine neoplasms. Neuroendocrine neoplasms share expression of somatostatin receptor type 2 with CD34-positive hematopoietic progenitor cells, potentially leading to active uptake in the radiosensitive red marrow region where these cells are located. This study aimed to identify and quantify specific red marrow uptake using SPECT/CT images collected after the first treatment cycle. Seventeen patients diagnosed with neuroendocrine neoplasms were treated with [Lu]Lu-DOTATATE. Seven of them had confirmed bone metastases. After the first treatment cycle, each patient went through 4 SPECT/CT imaging sessions 4, 24, 48, and 168 h after administration. Monte Carlo-based reconstructions were used to quantify activity concentrations in tumors and multiple skeletal sites presumed to house red marrow: the T9-L5 vertebrae and the ilium portion of the hip bones. The activity concentration from the descending aorta was used as input in a compartment model intended to establish a pure red marrow biodistribution by separating the nonspecific blood-based contribution from the specific activity concentration in red marrow. The biodistributions from the compartment model were used to perform red marrow dosimetry at each skeletal site. Increased uptake of [Lu]Lu-DOTATATE was observed in the T9-L5 vertebrae and hip bones in all 17 patients compared with activity concentrations in the aorta. The mean specific red marrow uptake was 49% (range, 0%-93%) higher than the nonspecific uptake. The median (±SD) total absorbed dose to the red marrow was 0.056 ± 0.023 Gy/GBq and 0.043 ± 0.022 Gy/GBq for the mean of all vertebrae and hip bones, respectively. The patients with bone metastases had an absorbed dose of 0.085 ± 0.046 Gy/GBq and 0.069 ± 0.033 Gy/GBq for the vertebrae and hip bones, respectively. The red marrow elimination phase was statistically slower in patients with fast tumor elimination, which is in line with transferrin transport of Lu back to the red marrow. Our results suggest that specific red marrow uptake of [Lu]Lu-DOTATATE is in line with observations of somatostatin receptor type 2-expressing hematopoietic progenitor cells within the bone marrow. Blood-based dosimetry methods fail to account for the prolonged elimination of specific uptake and underestimate the absorbed dose to red marrow.
骨髓抑制是神经内分泌肿瘤患者接受 [Lu]Lu-DOTATATE 治疗后的常见副作用。神经内分泌肿瘤与 CD34 阳性造血祖细胞共同表达生长抑素受体 2,这可能导致放射性敏感的红骨髓区域内的放射性摄取增加,而这些细胞就位于红骨髓区域内。本研究旨在使用首次治疗周期后采集的 SPECT/CT 图像来识别和量化特定的红骨髓摄取。
17 名被诊断患有神经内分泌肿瘤的患者接受了 [Lu]Lu-DOTATATE 治疗。其中 7 名患者已确认存在骨转移。在首个治疗周期后,每位患者在给药后 4、24、48 和 168 小时分别进行了 4 次 SPECT/CT 成像。采用基于蒙特卡罗的重建方法来量化肿瘤和多个被认为包含红骨髓的骨骼部位的活性浓度:T9-L5 椎体和髋骨的髂骨部分。将降主动脉的活性浓度用作房室模型的输入,该模型旨在通过从红骨髓中的特异性活性浓度中分离出非特异性血液贡献来建立纯红骨髓的生物分布。从房室模型获得的生物分布用于在每个骨骼部位进行红骨髓剂量计算。
与主动脉中的活性浓度相比,所有 17 名患者的 T9-L5 椎体和髋骨中均观察到 [Lu]Lu-DOTATATE 的摄取增加。特异性红骨髓摄取的平均百分比(范围:0%-93%)比非特异性摄取高 49%。所有椎体和髋骨的平均总吸收剂量分别为 0.056±0.023 Gy/GBq 和 0.043±0.022 Gy/GBq。存在骨转移的患者的椎体和髋骨的吸收剂量分别为 0.085±0.046 Gy/GBq 和 0.069±0.033 Gy/GBq。对于肿瘤清除较快的患者,红骨髓清除相的统计学上较慢,这与 Lu 通过转铁蛋白返回红骨髓的转运一致。
我们的结果表明,[Lu]Lu-DOTATATE 的特异性红骨髓摄取与骨髓中表达生长抑素受体 2 的造血祖细胞的观察结果一致。基于血液的剂量计算方法无法解释特异性摄取的延长清除,并且低估了红骨髓的吸收剂量。