Rheumatology Unit, First Department of Propaedeutic Internal Medicine, Joint Academic Rheumatology Program, Laiko Hospital, Medical School, National and Kapodistrian University, Athens, Greece.
Department of Nephrology and Renal Transplantation, Laiko Hospital, Medical School, National and Kapodistrian University, Athens, Greece.
RMD Open. 2023 Jun;9(2). doi: 10.1136/rmdopen-2023-003158.
A preliminary definition of disease modification (DM) in lupus nephritis (LN) was recently developed focusing on long-term remission and damage prevention, with minimal treatment-associated toxicity. We aimed to further specify aspects of DM criteria in LN, assess DM achievement in a real-world setting and examine potential DM predictors and long-term outcomes.
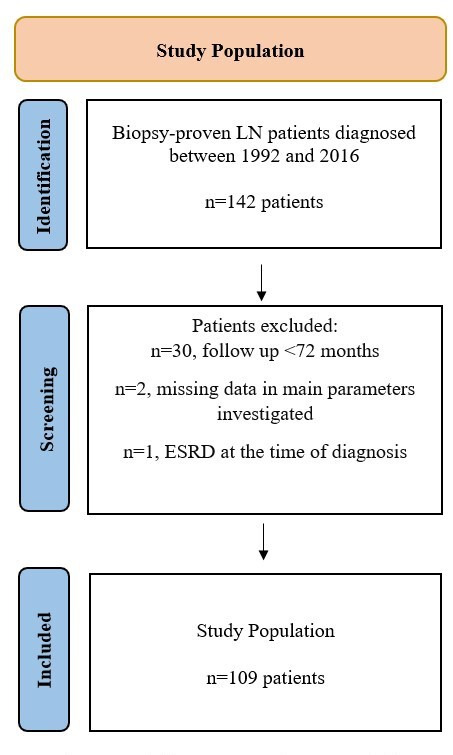
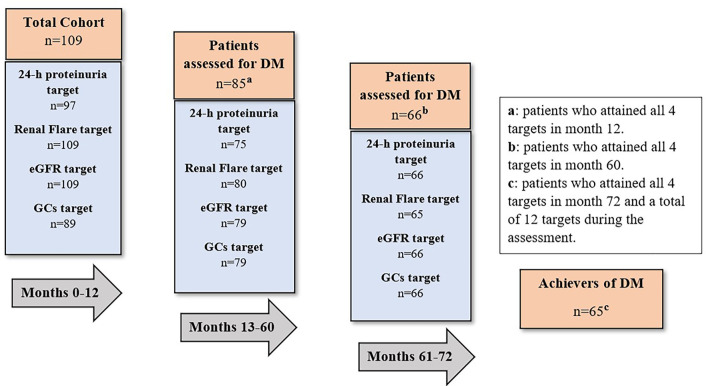
We collected clinical/laboratory and histological inception cohort data from biopsy-proven LN patients (82% females) with ≥72 months follow-up at two joint academic centres. Specific criteria for 24-hour proteinuria, estimated glomerular filtration rate (eGFR), renal flares and glucocorticoids dose were set at three time frames (months 0-12, 13-60 and 72) to assess DM. In the first model, DM was achieved if patients fulfilled all four criteria at all three time frames (achievers). In the second model, the continued glucocorticoids reduction criterion was excluded. Logistic regression analyses were performed. Possible different trends in DM achievement between past and recent decades were also investigated.
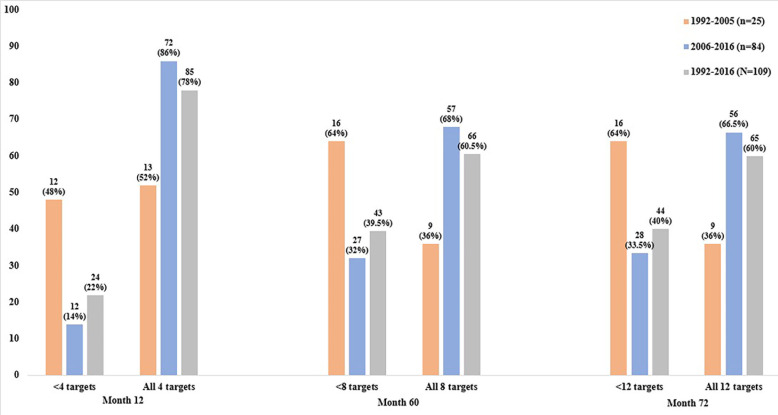
DM was achieved by 60% of patients, increased to 70% when glucocorticoids excluded from DM criteria. 24-hour proteinuria at 9 months predicted DM achievement (OR 0.72, 95% CI 0.53 to 0.97, p=0.03), but none of baseline characteristics. Among patients with >72 month follow-up, non-achievers had worse renal outcomes (flares, >30% proteinuria increase, eGFR decline) than achievers at the end of follow-up (median 138 months). Patients diagnosed between 1992 and 2005 were found to have significantly lower percentages of DM achievement and met less often the glucocorticoids dose reduction criterion in all three time frames, compared with those diagnosed between 2006 and 2016 (p=0.006 and p<0.01, respectively).
DM was achieved by only 60% of LN patients in a real-life setting, partly due to lack of glucocorticoids dose target attainment, while DM failure was associated with worse long-term renal outcomes. This may imply limitations in the effectiveness or implementation of current LN treatments, supporting the need for novel therapeutic strategies.
最近针对长期缓解和预防损伤,提出了狼疮肾炎(LN)疾病修饰(DM)的初步定义,其重点是最小化与治疗相关的毒性。我们旨在进一步明确 LN 中 DM 标准的各个方面,评估真实环境中的 DM 实现情况,并探讨潜在的 DM 预测因素和长期结果。
我们从两家联合学术中心接受肾活检证实的 LN 患者(82%为女性)中收集了临床/实验室和组织学的发病队列数据,随访时间≥72 个月。在三个时间点(0-12 个月、13-60 个月和 72 个月)设定了 24 小时蛋白尿、估算肾小球滤过率(eGFR)、肾发作和糖皮质激素剂量的具体标准,以评估 DM。在第一个模型中,如果患者在所有三个时间点都满足所有四个标准,则认为达到 DM(达标者)。在第二个模型中,排除了持续减少糖皮质激素的标准。进行了逻辑回归分析。还研究了过去和最近几十年 DM 实现之间可能存在的不同趋势。
60%的患者达到 DM,当将糖皮质激素排除在 DM 标准之外时,达到 DM 的比例增加到 70%。9 个月时的 24 小时蛋白尿预测 DM 的实现(OR 0.72,95%CI 0.53 至 0.97,p=0.03),但基线特征均无预测作用。在随访时间超过 72 个月的患者中,未达标者在随访结束时(中位时间 138 个月)的肾脏结局(发作、蛋白尿增加>30%、eGFR 下降)比达标者更差。与 2006 年至 2016 年诊断的患者相比,1992 年至 2005 年诊断的患者达到 DM 的百分比明显较低,并且在所有三个时间点均较少满足糖皮质激素剂量减少的标准(p=0.006 和 p<0.01)。
在真实环境中,只有 60%的 LN 患者达到 DM,部分原因是缺乏糖皮质激素剂量目标的实现,而 DM 失败与长期肾脏结局恶化有关。这可能意味着当前 LN 治疗的有效性或实施存在局限性,支持需要新的治疗策略。