Oliveira Marília, Rahawi Kassim, Duan Yinghui, Lane Michael, Amin Ahmad Z, Sayed Christopher J
US Medical Affairs Dermatology, AbbVie Inc., North Chicago, IL, USA.
US Medical Affairs Oncology, AbbVie Inc., North Chicago, IL, USA.
Dermatol Ther (Heidelb). 2023 Jul;13(7):1577-1585. doi: 10.1007/s13555-023-00954-8. Epub 2023 Jun 14.
Management of hidradenitis suppurativa (HS) often requires a combined medical/procedural approach. Biologics are frequently reserved for severe cases after irreversible tissue damage has occurred. We evaluated the association between consistent biologic use and the need for procedural interventions, systemic medications, and healthcare utilization.
UNITE, a 4-year, global, prospective, observational, HS disease registry, documented the natural history, diagnostic/treatment patterns, and clinical outcomes of HS. Patients aged 12 years or more, with active HS were enrolled between October 2013 and December 2015 and evaluated every 6 months for 48 months at 73 sites across 12 countries (data cutoff December 2019). Proportions of patients requiring different HS procedures, systemic medications, and healthcare utilization were assessed during the 6-month periods before, during, and after biologic initiation for 12 weeks or more (i.e., consistent use).
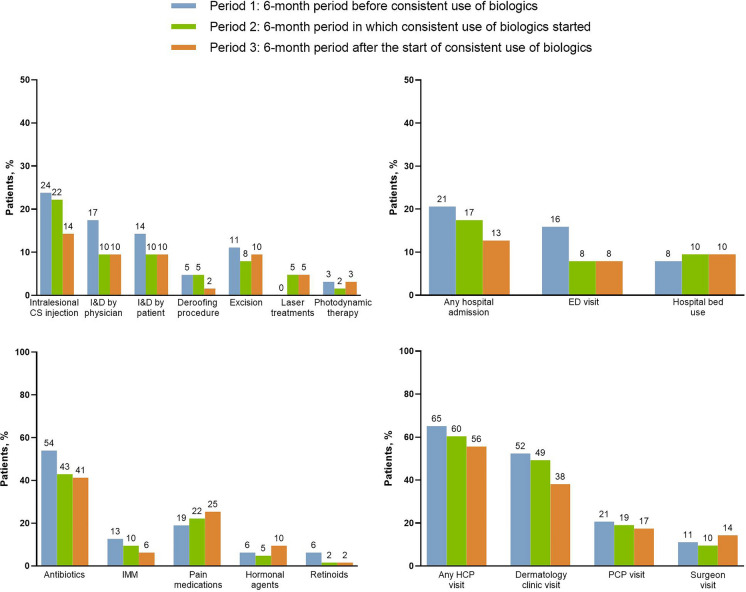
There were 63 instances of initiation of consistent biologic use (adalimumab [81%], infliximab [16%], and ustekinumab [3%]) in 57 patients. Patients' mean age was 40 years, 58% were female, and 53%/47% had Hurley stage II/III disease, respectively. Fewer patients required surgical/procedural interventions and systemic medications for the 6-month period during/6-month period after biologic initiation versus the 6-month period before biologic initiation, including intralesional corticosteroid injections (22%/14% vs 24%), incision and drainage (I&D) by physician (10%/10% vs 17%), I&D by patient (10%/10% vs 14%), surgical excision (8%/10% vs 11%), deroofing (5%/2% vs 5%), systemic antibiotics (43%/41% vs 54%), and systemic immunosuppressants (10%/6% vs 13%). Fewer patients required hospital admission for HS (17%/13% vs 21%) or emergency department visits for HS (8%/8% vs 16%) during the 6-month periods in which consistent biologics use started and continued versus the 6-month period before consistent biologic use.
Following initiation of consistent biologic use (12 weeks or more), fewer patients required acute procedural interventions, systemic medications, and healthcare utilization, supporting the importance of early biologic initiation.
化脓性汗腺炎(HS)的管理通常需要药物和手术相结合的方法。生物制剂通常用于组织发生不可逆损伤后的严重病例。我们评估了持续使用生物制剂与手术干预需求、全身用药及医疗资源利用之间的关联。
UNITE是一项为期4年的全球前瞻性观察性HS疾病登记研究,记录了HS的自然病史、诊断/治疗模式及临床结局。2013年10月至2015年12月期间纳入12岁及以上的活动性HS患者,并在12个国家的73个研究点每6个月进行一次评估,为期48个月(数据截止于2019年12月)。在开始使用生物制剂12周或更长时间(即持续使用)之前、期间及之后的6个月内,评估需要不同HS手术、全身用药及医疗资源利用的患者比例。
57例患者中有63次开始持续使用生物制剂(阿达木单抗[81%]、英夫利昔单抗[16%]、优特克单抗[3%])。患者的平均年龄为40岁,58%为女性,53%/47%分别处于Hurley II/III期疾病。与开始使用生物制剂前的6个月相比,在开始使用生物制剂期间的6个月/之后的6个月内,需要手术/手术干预和全身用药的患者更少,包括病灶内注射皮质类固醇(22%/14%对24%)、医生进行的切开引流(I&D)(10%/10%对17%)、患者自行进行的I&D(10%/10%对14%)、手术切除(8%/10%对11%)、去顶术(5%/2%对5%)、全身使用抗生素(43%/41%对54%)以及全身使用免疫抑制剂(10%/6%对13%)。在开始并持续使用生物制剂的6个月内,因HS需要住院治疗(17%/13%对21%)或前往急诊科就诊(8%/8%对16%)的患者比在开始持续使用生物制剂前的6个月更少。
在开始持续使用生物制剂(12周或更长时间)后,需要急性手术干预、全身用药及医疗资源利用的患者减少,这支持了早期使用生物制剂的重要性。