Department of Anesthesia, Critical Care, and Pain Medicine, Massachusetts General Hospital, Boston.
Department of Anesthesia, Harvard Medical School, Boston, Massachusetts.
JAMA Surg. 2023 Aug 1;158(8):854-864. doi: 10.1001/jamasurg.2023.2009.
Opioids administered to treat postsurgical pain are a major contributor to the opioid crisis, leading to chronic use in a considerable proportion of patients. Initiatives promoting opioid-free or opioid-sparing modalities of perioperative pain management have led to reduced opioid administration in the operating room, but this reduction could have unforeseen detrimental effects in terms of postoperative pain outcomes, as the relationship between intraoperative opioid usage and later opioid requirements is not well understood.
To characterize the association between intraoperative opioid usage and postoperative pain and opioid requirements.
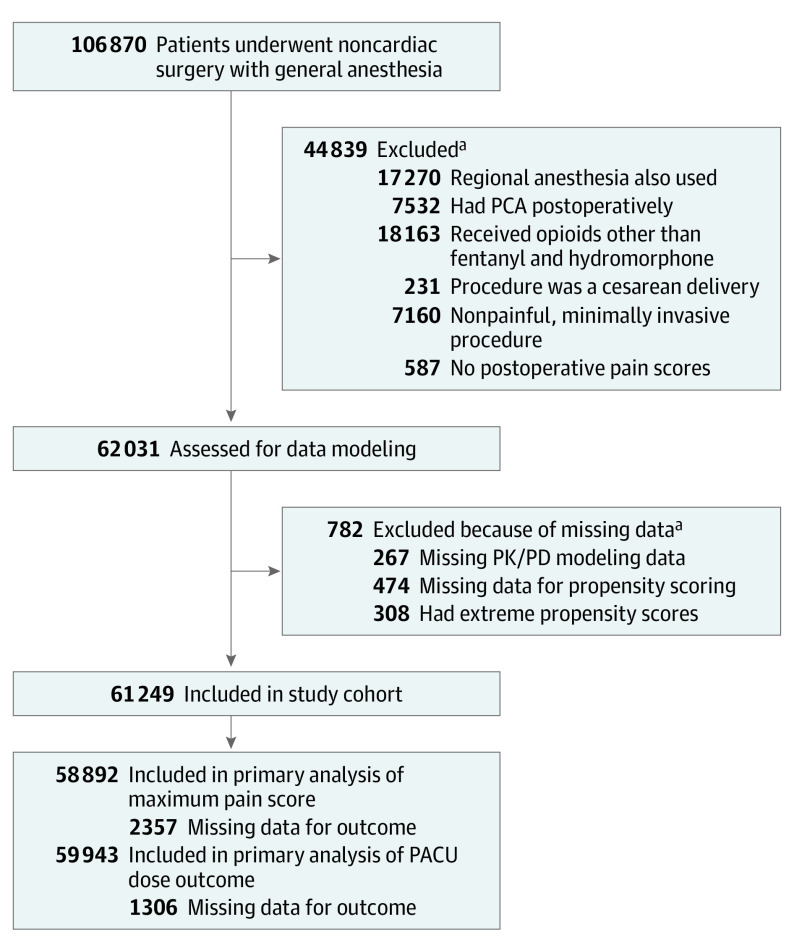
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study evaluated electronic health record data from a quaternary care academic medical center (Massachusetts General Hospital) for adult patients who underwent noncardiac surgery with general anesthesia from April 2016 to March 2020. Patients who underwent cesarean surgery, received regional anesthesia, received opioids other than fentanyl or hydromorphone, were admitted to the intensive care unit, or who died intraoperatively were excluded. Statistical models were fitted on the propensity weighted data set to characterize the effect of intraoperative opioid exposures on primary and secondary outcomes. Data were analyzed from December 2021 to October 2022.
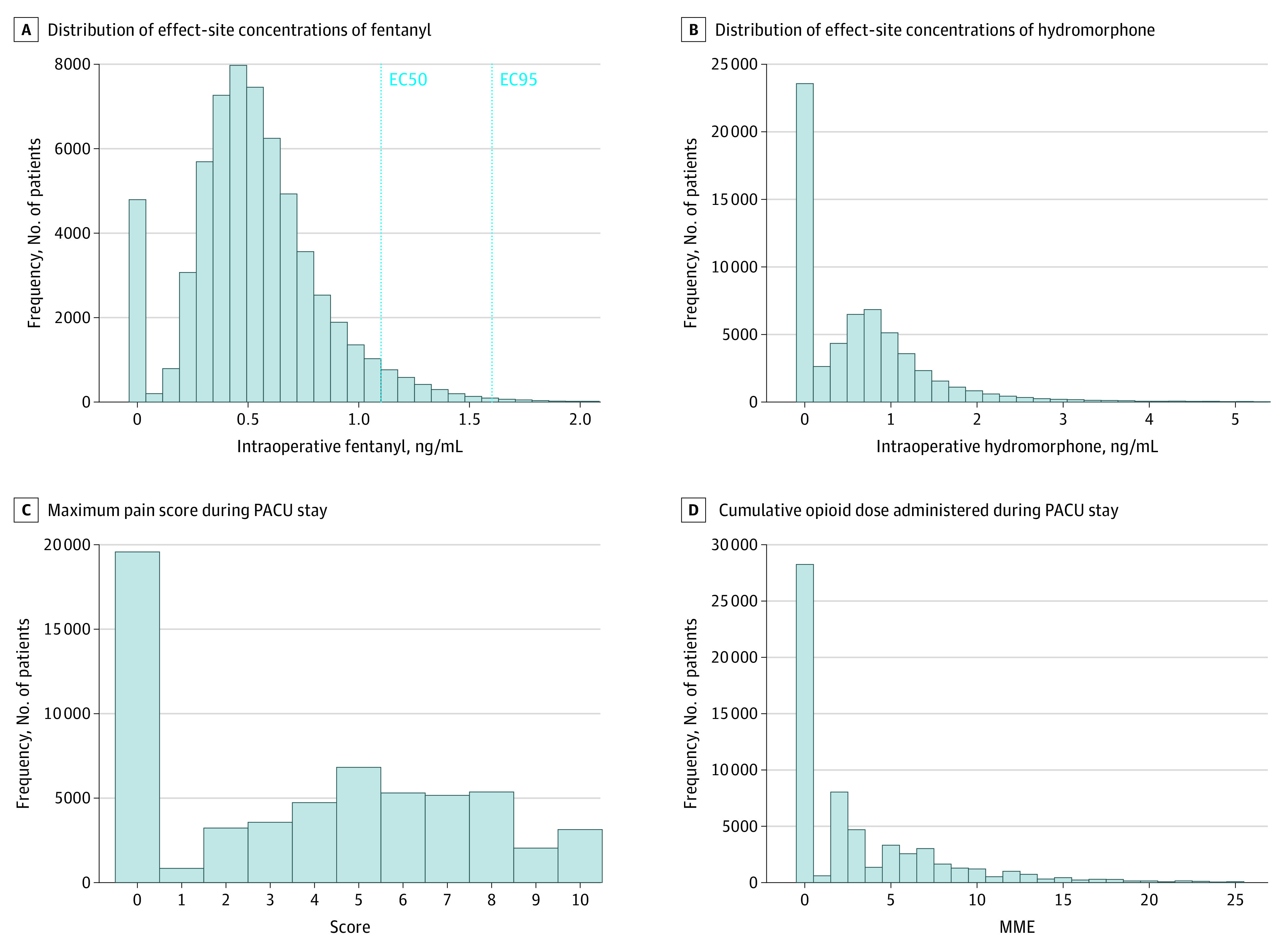
Intraoperative fentanyl and intraoperative hydromorphone average effect site concentration estimated using pharmacokinetic/pharmacodynamic models.
The primary study outcomes were the maximal pain score during the postanesthesia care unit (PACU) stay and the cumulative opioid dose, quantified in morphine milligram equivalents (MME), administered during the PACU stay. Medium- and long-term outcomes associated with pain and opioid dependence were also evaluated.
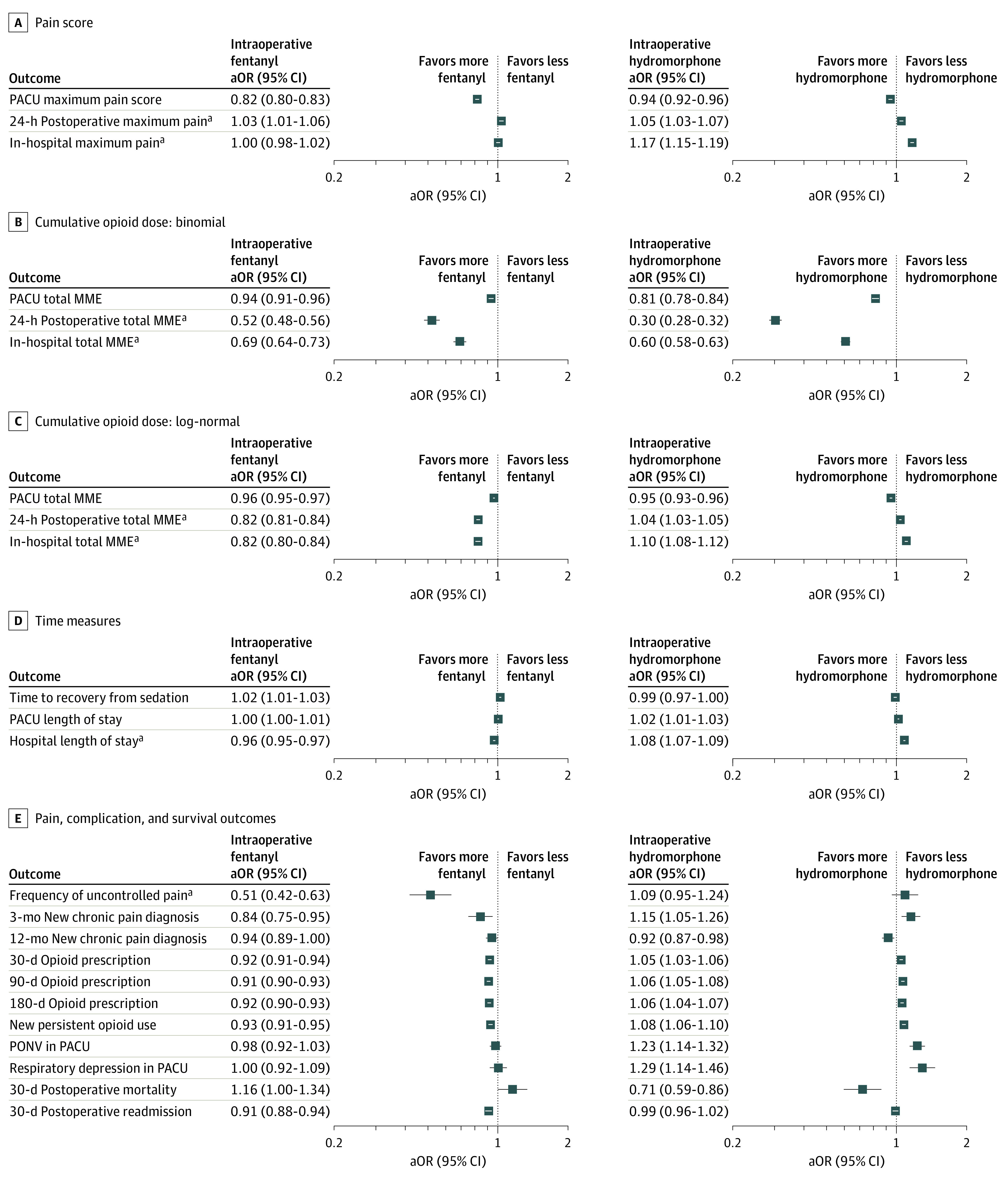
The study cohort included a total of 61 249 individuals undergoing surgery (mean [SD] age, 55.44 [17.08] years; 32 778 [53.5%] female). Increased intraoperative fentanyl and intraoperative hydromorphone were both associated with reduced maximum pain scores in the PACU. Both exposures were also associated with a reduced probability and reduced total dosage of opioid administration in the PACU. In particular, increased fentanyl administration was associated with lower frequency of uncontrolled pain; a decrease in new chronic pain diagnoses reported at 3 months; fewer opioid prescriptions at 30, 90, and 180 days; and decreased new persistent opioid use, without significant increases in adverse effects.
Contrary to prevailing trends, reduced opioid administration during surgery may have the unintended outcome of increasing postoperative pain and opioid consumption. Conversely, improvements in long-term outcomes might be achieved by optimizing opioid administration during surgery.
用于治疗术后疼痛的阿片类药物是阿片类药物危机的主要原因,导致相当一部分患者出现慢性使用。提倡围手术期疼痛管理的无阿片类药物或减少阿片类药物的模式,导致手术室中阿片类药物的使用减少,但这一减少可能会对术后疼痛结果产生意想不到的不利影响,因为术中阿片类药物使用与后期阿片类药物需求之间的关系尚未得到很好的理解。
描述术中阿片类药物使用与术后疼痛和阿片类药物需求之间的关系。
设计、设置和参与者:这项回顾性队列研究评估了来自一家四等医疗学术医疗中心(马萨诸塞州总医院)的电子健康记录数据,该中心的成年患者在 2016 年 4 月至 2020 年 3 月期间接受全身麻醉下的非心脏手术。排除接受剖宫产手术、接受区域麻醉、接受芬太尼或氢吗啡酮以外的阿片类药物、入住重症监护病房或术中死亡的患者。在倾向加权数据集上拟合统计模型,以描述术中阿片类药物暴露对主要和次要结果的影响。数据于 2021 年 12 月至 2022 年 10 月进行分析。
使用药代动力学/药效学模型估计术中芬太尼和术中氢吗啡酮的平均效应部位浓度。
主要研究结果是 PACU 期间的最大疼痛评分和 PACU 期间给予的吗啡毫克当量(MME)累积阿片类药物剂量。还评估了与疼痛和阿片类药物依赖相关的中、长期结果。
研究队列共包括 61249 名接受手术的患者(平均[标准差]年龄为 55.44[17.08]岁;32778[53.5%]为女性)。术中芬太尼和氢吗啡酮的增加均与 PACU 中最大疼痛评分降低相关。两种暴露均与 PACU 中阿片类药物给药的概率和总剂量降低相关。特别是,芬太尼的使用与无控制疼痛的频率降低有关;3 个月时报告的新慢性疼痛诊断减少;30、90 和 180 天时的阿片类药物处方减少;以及新的持续性阿片类药物使用减少,而不良事件没有明显增加。
与流行趋势相反,手术期间减少阿片类药物的使用可能会导致术后疼痛和阿片类药物使用增加的意外后果。相反,通过优化手术期间的阿片类药物管理,可能会实现长期结果的改善。