Xu Shao-Jun, Chen Rui-Qin, Tu Jia-Hua, You Cheng-Xiong, Chen Chao, Zhang Zhi-Fan, Divisi Duilio, Migliore Marcello, Bongiolatti Stefano, Durand Marion, Sato Masaaki, Kuroda Hiroaki, Yang Chao-Fu, Yu Shao-Bin, Chen Shu-Chen
Department of Thoracic Surgery, Fujian Medical University Union Hospital, Fuzhou, China.
Key Laboratory of Ministry of Education for Gastrointestinal Cancer, Fujian Medical University, Fuzhou, China.
Transl Lung Cancer Res. 2023 May 31;12(5):1078-1092. doi: 10.21037/tlcr-23-246. Epub 2023 May 24.
This study aimed to evaluate the effect of the presence of a radiographically manifested ground-glass opacity (GGO) component on the prognosis of patients with pathological stage IA3 lung adenocarcinoma.
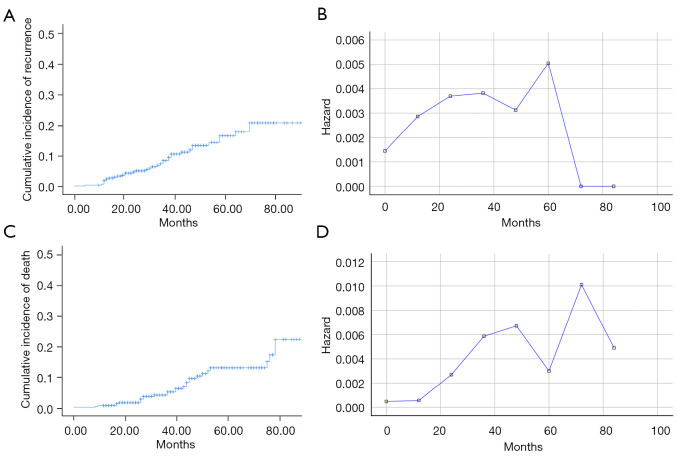
Patients diagnosed with pathological stage IA3 lung adenocarcinoma who underwent radical surgery at two medical institutions in China between July 2012 and July 2020 were enrolled. The cumulative incidence of recurrence (CIR) and cumulative incidence of death (CID) in patients with and without a GGO component were compared. Risk curves for the recurrence and tumor-related death overtime were analyzed between the two groups according to life table. In order to validate the prognostic value of GGO components, the recurrence-free survival (RFS) and cancer-specific survival (CSS) were estimated. Decision curve analysis (DCA) was performed to evaluate the clinical benefit rate of different models.
Among the 352 included patients, the presence of a GGO component was radiographically shown in 166 (47.2%) patients, while 186 (52.8%) displayed solid nodules. Patients exhibiting the absence of a GGO component had higher incidences of total recurrence (17.2% 3.0%, P<0.001), local-regional recurrence (LRR) (5.4% 0.6%, P=0.010), distant metastasis (DM) (8.1% 1.8%, P=0.008), and multiple recurrences (4.3% 0.6%, P=0.028) than the presence-GGO component group. The 5-year CIR and CID were 7.5% and 7.4% in the presence-GGO component group, and 24.5% and 17.0% in the absence-GGO component group, respectively, with statistically significant differences between the two groups (P<0.05). The risk of recurrence in patients with the presence of GGO components showed a single peak at 3 years postoperatively, while patients with the absence of GGO components showed a double peak at 1 and 5 years after surgery, respectively. However, the risk of tumor-related death peaked in both groups at 3 and 6 years postoperatively. Multivariate Cox analysis showed that the presence of a GGO component was a favorable independent risk factor for pathological stage IA3 lung adenocarcinoma patients (P<0.05).
Pathological stage IA3 lung adenocarcinoma with or without GGO components are two types of tumors with different invasive abilities. In clinical practice, we should develop different treatment and follow-up strategies.
本研究旨在评估影像学表现为磨玻璃影(GGO)成分对病理IA3期肺腺癌患者预后的影响。
纳入2012年7月至2020年7月在中国两家医疗机构接受根治性手术的病理IA3期肺腺癌患者。比较有和无GGO成分患者的复发累积发生率(CIR)和死亡累积发生率(CID)。根据生命表分析两组患者复发和肿瘤相关死亡随时间的风险曲线。为验证GGO成分的预后价值,估计无复发生存期(RFS)和癌症特异性生存期(CSS)。进行决策曲线分析(DCA)以评估不同模型的临床获益率。
在纳入的352例患者中,166例(47.2%)影像学显示有GGO成分,186例(52.8%)表现为实性结节。无GGO成分的患者总复发率(17.2% 对3.0%,P<0.001)、局部区域复发率(LRR)(5.4% 对0.6%,P=0.010)、远处转移率(DM)(8.1% 对1.8%,P=0.008)和多次复发率(4.3% 对0.6%,P=0.028)均高于有GGO成分组。有GGO成分组的5年CIR和CID分别为7.5%和7.4%,无GGO成分组分别为24.5%和17.0%,两组间差异有统计学意义(P<0.05)。有GGO成分的患者术后3年复发风险出现单峰,无GGO成分的患者术后1年和5年分别出现双峰。然而,两组肿瘤相关死亡风险均在术后3年和6年达到峰值。多因素Cox分析显示,GGO成分的存在是病理IA3期肺腺癌患者的有利独立危险因素(P<0.05)。
有或无GGO成分的病理IA3期肺腺癌是两种具有不同侵袭能力的肿瘤类型。在临床实践中,应制定不同的治疗和随访策略。