Downing Maren, Modrow Michael, Thompson-Brazill Kelly A, Ledford J Erin, Harr Charles D, Williams Judson B
WakeMed Health and Hospitals, Raleigh, NC.
Campbell University School of Osteopathic Medicine, Lillington, NC.
JTCVS Tech. 2023 Apr 14;19:93-103. doi: 10.1016/j.xjtc.2023.03.019. eCollection 2023 Jun.
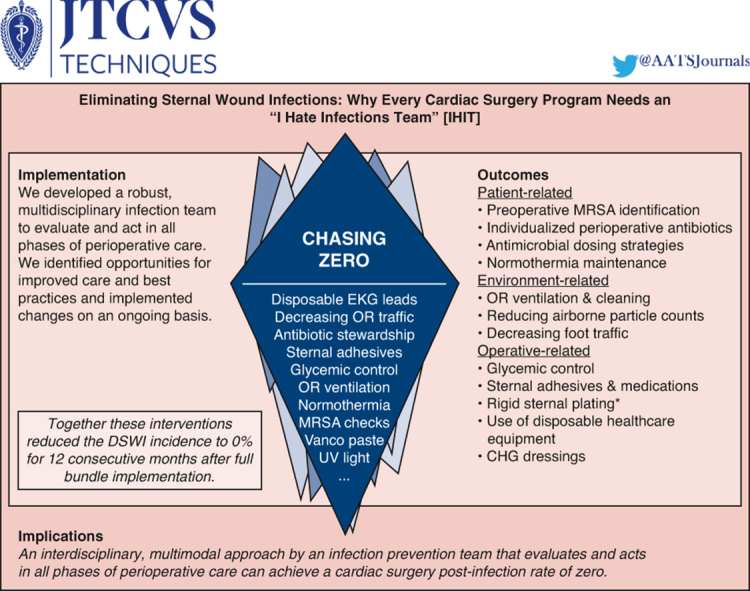
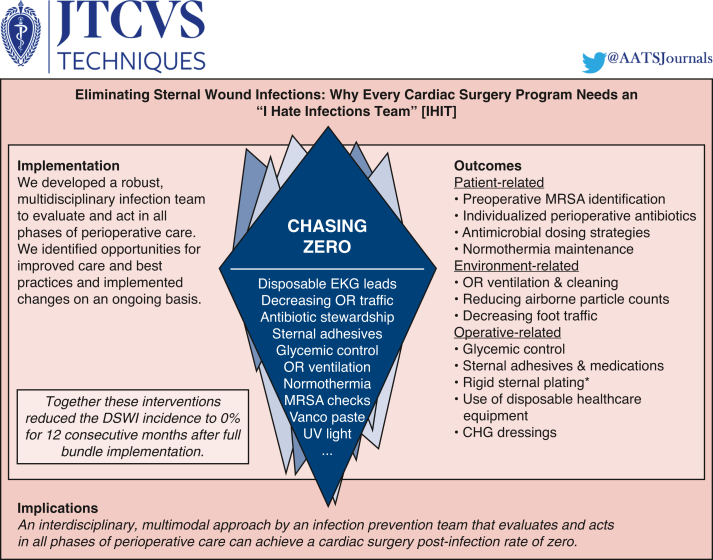
The majority of studies examining deep sternal wound infection (DSWI) prevention focus on ameliorating 1 variable at a time. There is a paucity of data regarding the synergistic effects of combining clinical and environmental interventions. This article describes an interdisciplinary, multimodal approach to eliminate DSWIs at a large community hospital.
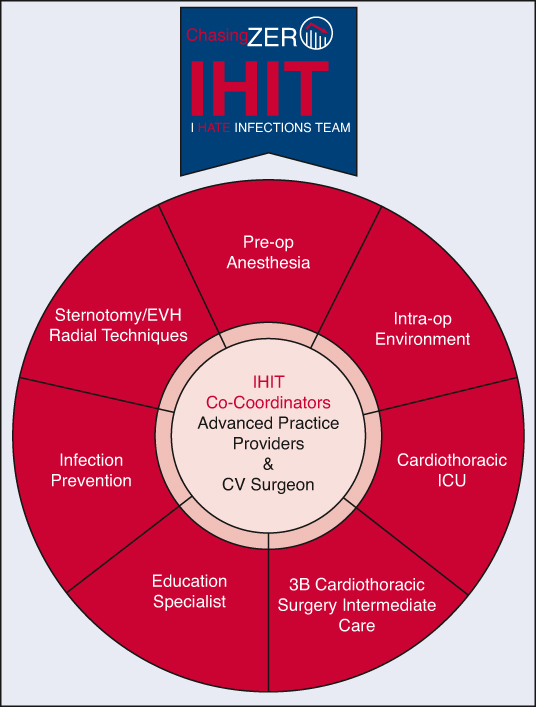
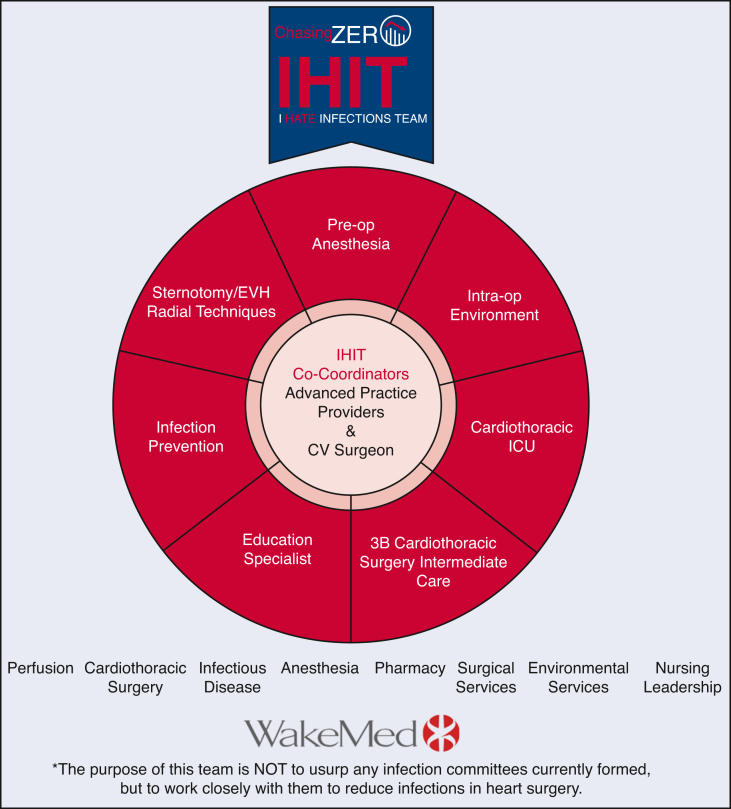
We developed a robust, multidisciplinary infection prevention team to evaluate and act in all phases of perioperative care to achieve a cardiac surgery DSWI rate of 0, named: the I hate infections team. The team identified opportunities for improved care and best practices and implemented changes on an ongoing basis.
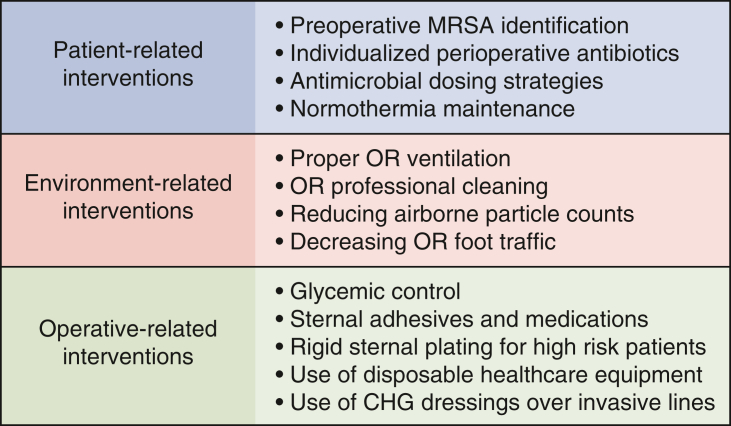
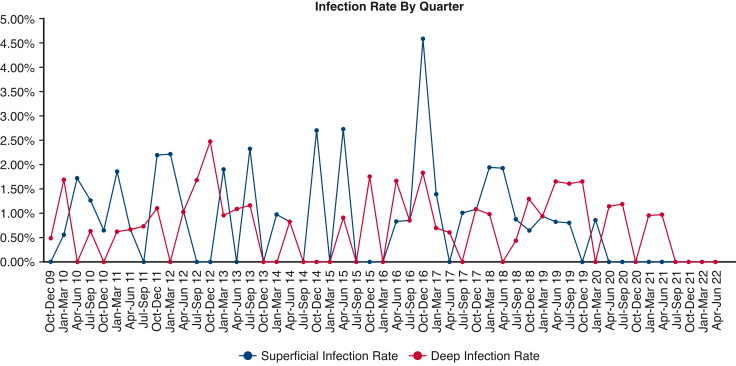
Patient-related interventions consisted of preoperative methicillin-resistant identification, individualized perioperative antibiotics, antimicrobial dosing strategies, and maintenance of normothermia. Operative-related interventions involved glycemic control, sternal adhesives, medications and hemostasis, rigid sternal fixation for high-risk patients, chlorhexidine gluconate dressings over invasive lines, and use of disposable health care equipment. Environment-related interventions included optimizing operating room ventilation and terminal cleaning, reducing airborne particle counts, and decreasing foot traffic. Together, these interventions reduced the DSWI incidence from 1.6% preintervention to 0% for 12 consecutive months after full bundle implementation.
A multidisciplinary team focused on eliminating DSWI identified known risk factors and implemented evidence-based interventions in each phase of care to ameliorate risk. Although the influence of each individual intervention on DSWI remains unknown, use of the bundled infection prevention approach reduced the incidence to 0 for the first 12 months after implementation.
大多数关于预防深部胸骨伤口感染(DSWI)的研究一次只关注改善一个变量。关于临床和环境干预相结合的协同效应的数据很少。本文描述了一家大型社区医院采用的跨学科、多模式方法来消除DSWI。
我们组建了一个强大的多学科感染预防团队,在围手术期护理的各个阶段进行评估并采取行动,以实现心脏手术DSWI发生率为0,该团队名为:我讨厌感染团队。该团队确定了改善护理的机会和最佳实践,并持续进行改进。
与患者相关的干预措施包括术前耐甲氧西林菌鉴定、个体化围手术期抗生素、抗菌药物给药策略以及维持正常体温。与手术相关的干预措施包括血糖控制、胸骨粘合剂、药物和止血、高危患者的坚固胸骨固定、在侵入性导管上使用葡萄糖酸洗必泰敷料以及使用一次性医疗设备。与环境相关的干预措施包括优化手术室通风和终末清洁、减少空气中的颗粒计数以及减少人员流动。这些干预措施共同作用,使DSWI发生率从干预前的1.6%降至全面实施综合措施后的连续12个月为0%。
一个专注于消除DSWI的多学科团队识别出已知的风险因素,并在护理的每个阶段实施基于证据的干预措施以降低风险。虽然每个单独干预措施对DSWI的影响尚不清楚,但采用综合感染预防方法在实施后的前12个月将发生率降至0。