Bhamidipati Castigliano M, Tohill Beth C, Robe Charee, Reid Kimberly J, Eglitis Nicholas C, Farber Mark A, Jordan William D
Division of Cardiothoracic Surgery, Department of Surgery, Oregon Health & Science University, Portland, OR.
W.L. Gore & Associates, Flagstaff, AZ.
J Vasc Surg Cases Innov Tech. 2023 Apr 22;9(2):101174. doi: 10.1016/j.jvscit.2023.101174. eCollection 2023 Jun.
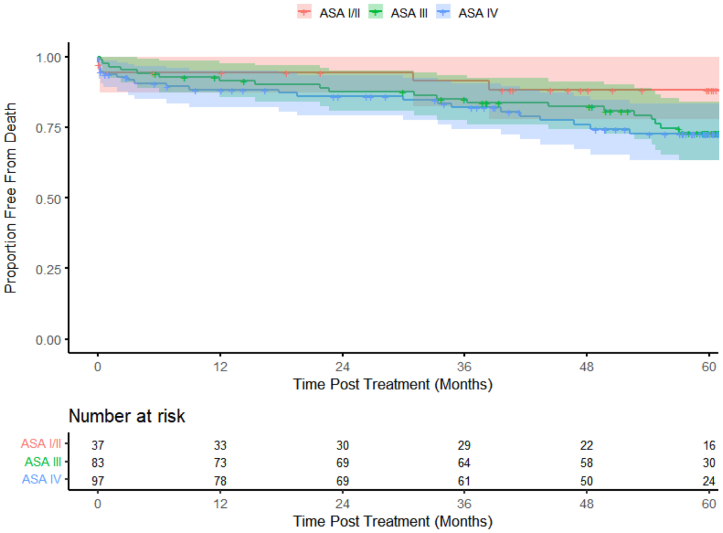
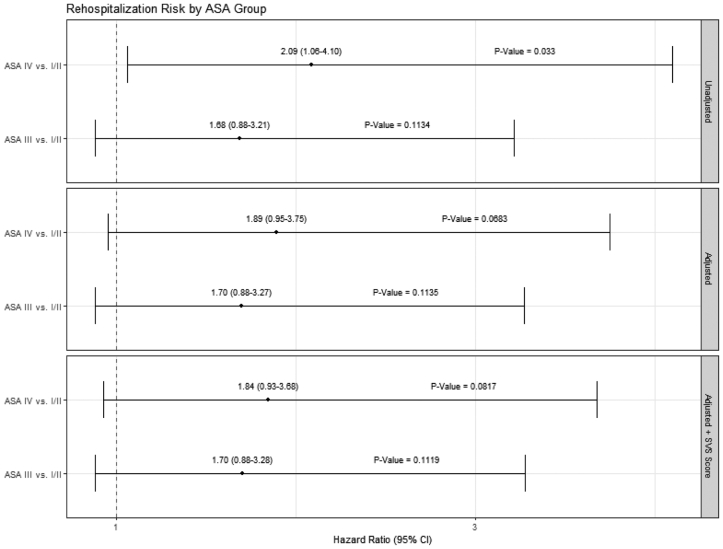
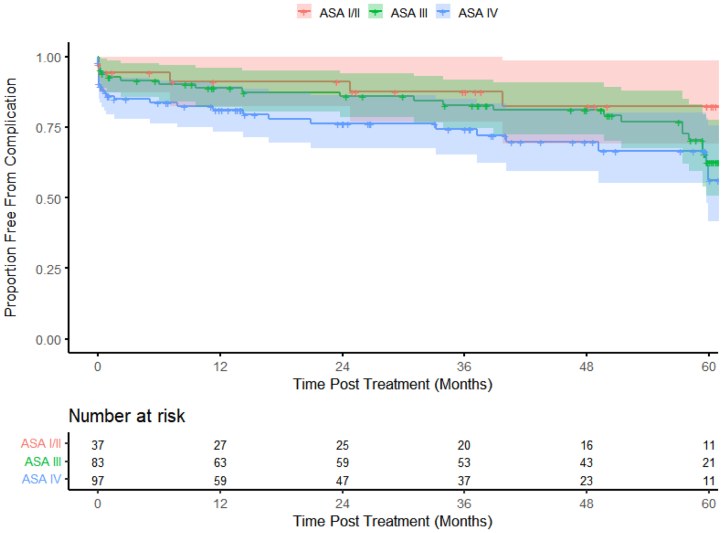
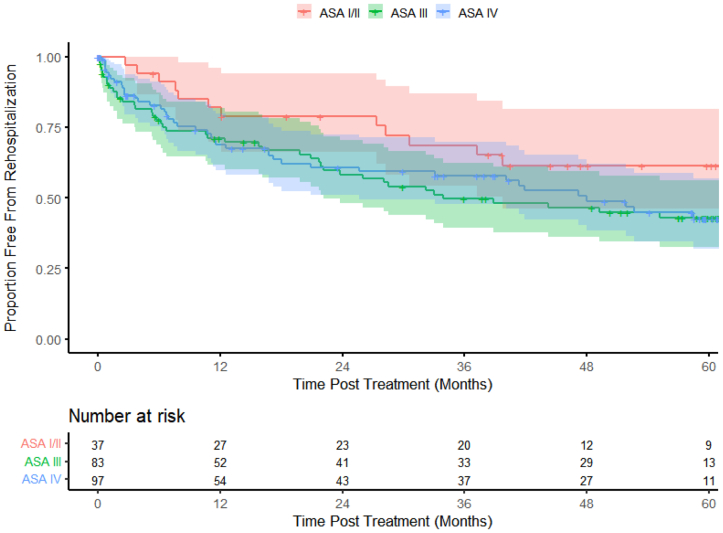
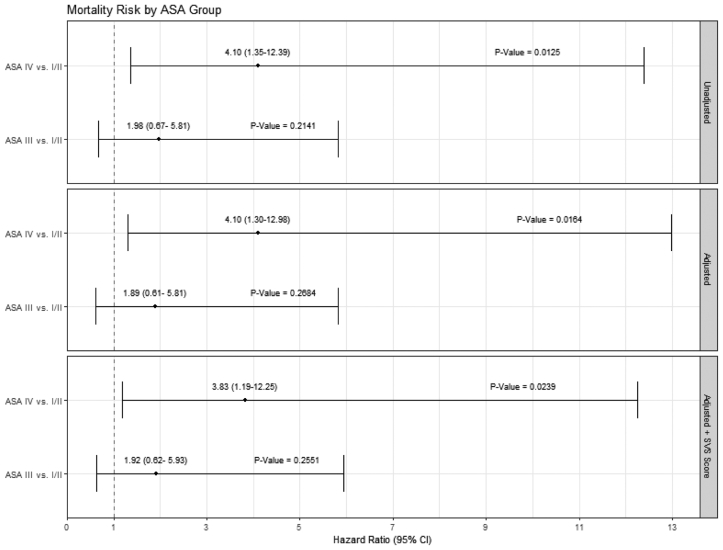
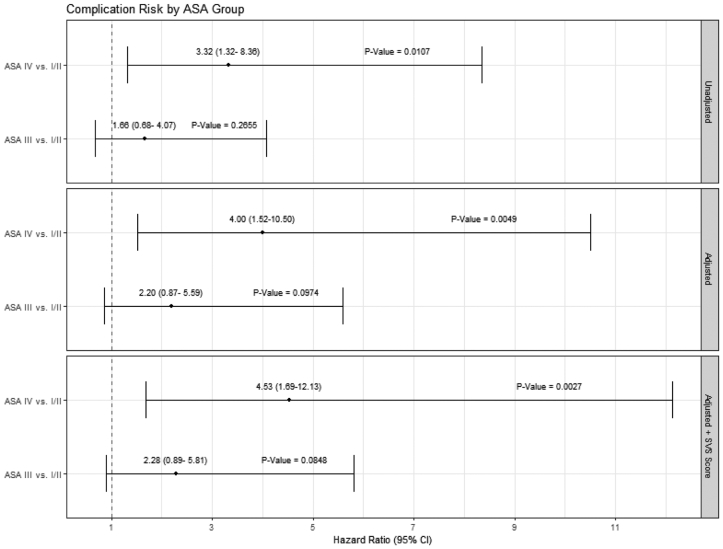
Use of the American Society of Anesthesiologists (ASA) physical status classification is important for periprocedural risk stratification. However, the collective effect after adjustment for the Society for Vascular Surgery (SVS) medical comorbidity grading system on long-term all-cause mortality, complications, and discharge disposition is unknown. We examined these associations in patients after thoracic endograft placement. Data from three thoracic endovascular aortic repair (TEVAR) trials through 5 years of follow-up were included. Patients with acute complicated type B dissection (n = 50), traumatic transection (n = 101), or descending thoracic aneurysm (n = 66) were analyzed. The patients were stratified into three groups according to the ASA class: I-II, III, and IV. Multivariable proportional hazards regression models were used to examine the effect of ASA class on 5-year mortality, complications, and rehospitalizations after adjustment for SVS risk score and potential confounders. The largest proportion of patients treated by TEVAR across the ASA groups (n = 217) was ASA IV (n = 97; 44.7%; < .001), followed by ASA III (n = 83; 38.2%) and ASA I-II (n = 37; 17.1%). Among the ASA groups, the ASA I-II patients were, on average, 6 years younger than those with ASA III and 3 years older than those with ASA IV (ASA I-II: age, 54.3 ± 22.0 years; ASA III: age, 60.0 ± 19.7 years; ASA IV: age, 51.0 ± 18.4 years; = .009). Multivariable adjusted 5-year outcome models showed that ASA class IV, independent of the SVS score, conferred an increased risk of mortality (hazard ratio [HR], 3.83; 95% confidence interval [CI], 1.19-12.25; = .0239) and complications (HR, 4.53; 95% CI, 1.69-12.13; = .0027) but not rehospitalization (HR, 1.84; 95% CI, 0.93-3.68; = .0817) compared with ASA class I-II. Procedural ASA class is associated with long-term outcomes among post-TEVAR patients, independent of the SVS score. The ASA class and SVS score remain important to patient counseling and postoperative outcomes beyond the index operation.
美国麻醉医师协会(ASA)身体状况分类的使用对于围手术期风险分层很重要。然而,在调整血管外科学会(SVS)合并症分级系统后,其对长期全因死亡率、并发症及出院处置的综合影响尚不清楚。我们研究了胸主动脉覆膜支架置入术后患者的这些关联。纳入了三项胸主动脉腔内修复术(TEVAR)试验5年随访的数据。分析了急性复杂性B型夹层(n = 50)、创伤性横断(n = 101)或降主动脉瘤(n = 66)患者。根据ASA分级将患者分为三组:I-II级、III级和IV级。使用多变量比例风险回归模型,在调整SVS风险评分和潜在混杂因素后,研究ASA分级对5年死亡率、并发症及再次住院的影响。在所有ASA组中接受TEVAR治疗的患者中,比例最大的是ASA IV级(n = 97;44.7%;P <.001),其次是ASA III级(n = 83;38.2%)和ASA I-II级(n = 37;17.1%)。在ASA组中,ASA I-II级患者平均比ASA III级患者年轻六岁,比ASA IV级患者大三岁(ASA I-II级:年龄,54.3±22.0岁;ASA III级:年龄,60.0±19.7岁;ASA IV级:年龄,51.0±18.4岁;P =.009)。多变量调整后的5年结局模型显示,与ASA I-II级相比,独立于SVS评分的ASA IV级会增加死亡风险(风险比[HR],3.83;95%置信区间[CI],1.19 - 12.25;P =.0239)和并发症风险(HR,4.53;95%CI,1.69 - 12.13;P =.0027),但不会增加再次住院风险(HR,1.84;95%CI,0.93 - 3.68;P =.081)。手术时的ASA分级与TEVAR术后患者的长期结局相关,独立于SVS评分。ASA分级和SVS评分对于患者咨询及索引手术之外的术后结局仍然很重要。