Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea.
Corneal Dystrophy Research Institute, Yonsei University College of Medicine, Seoul, Korea.
Korean J Ophthalmol. 2023 Aug;37(4):340-347. doi: 10.3341/kjo.2023.0032. Epub 2023 Jun 19.
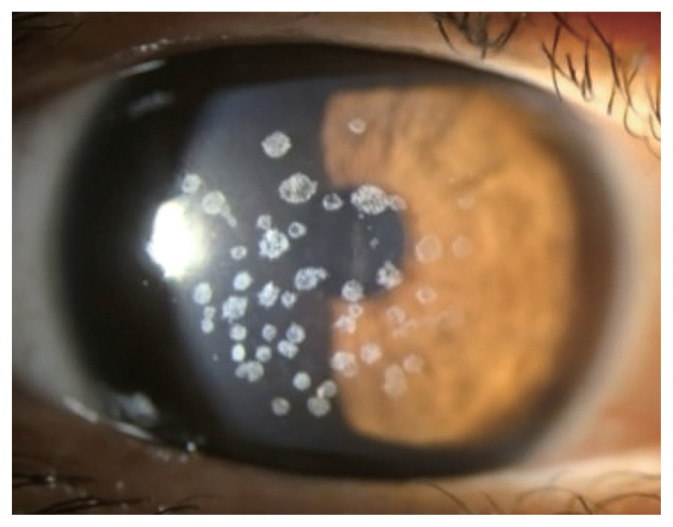
Granular corneal dystrophy type 2 (GCD2) is an autosomal dominant corneal stromal dystrophy that is caused by p.Arg124His mutation of transforming growth factor β induced (TGFBI) gene. It is characterized by well demarcated granular shaped opacities in central anterior stroma and as the disease progresses, extrusion of the deposits results in ocular pain due to corneal epithelial erosion. Also, diffuse corneal haze which appears late, causes decrease in visual acuity. The prevalence of GCD2 is high in East Asia including Korea. Homozygous patients show a severe phenotype from an early age, and the heterozygote phenotype varies among patients, depending on several types of compound heterozygous TGFBI mutations. In the initial stage, conservative treatments such as artificial tears, antibiotic eye drops, and bandage contact lenses are used to treat corneal erosion. Different surgical methods are used depending on the depth and extent of the stromal deposits. Phototherapeutic keratectomy removes anterior opacities and is advantageous in terms of its applicability and repeatability. For deeper lesions, deep anterior lamellar keratoplasty can be used as the endothelial layer is not always affected. Recurrence following these treatments are reported within a wide range of rates in different studies due to varying definition of recurrence and follow-up period. In patients who have undergone corneal laser vision-correction surgeries such as photorefractive keratectomy, LASEK, or LASIK including SMILE surgery, corneal opacity exacerbates rapidly with severe deterioration of visual acuity. Further investigations on new treatments of GCD2 are necessary.
2 型颗粒状角膜营养不良(GCD2)是一种常染色体显性角膜基质营养不良,由转化生长因子β诱导(TGFBI)基因突变引起。其特征是中央前角膜基质中边界清楚的颗粒状混浊,随着疾病的进展,由于角膜上皮侵蚀,沉积物的挤出导致眼部疼痛。此外,出现较晚的弥漫性角膜混浊导致视力下降。GCD2 在东亚包括韩国的患病率很高。纯合子患者从早期就表现出严重的表型,而杂合子表型因几种类型的复合 TGFBI 突变而异。在初始阶段,使用人工泪液、抗生素眼药水和绷带隐形眼镜等保守治疗来治疗角膜侵蚀。根据基质沉积物的深度和范围,采用不同的手术方法。光动力角膜切削术可去除前混浊,具有适用性和可重复性的优势。对于较深的病变,可以使用深层前板层角膜移植术,因为内皮层并不总是受到影响。由于不同研究中对复发的定义和随访期不同,这些治疗后的复发率报告范围很广。在接受过角膜激光视力矫正手术(如光折射性角膜切削术、LASEK 或 LASIK 手术,包括 SMILE 手术)的患者中,角膜混浊会迅速加重,视力严重恶化。需要进一步研究 GCD2 的新治疗方法。