Department of Cardiology, Hadassah Medical Center, Faculty of Medicine (Planer, Amir, Elbaz-Greener, Raccah) Hebrew University of Jerusalem, Israel; Division of Clinical Pharmacy, Institute for Drug Research, School of Pharmacy, Faculty of Medicine (Yanko, Matok, Zmiro, Rotshild, Raccah), Hebrew University of Jerusalem, Israel; Braun School of Public Health and Department of Hematology, Faculty of Medicine (Paltiel), Hebrew University of Jerusalem, Israel.
Department of Cardiology, Hadassah Medical Center, Faculty of Medicine (Planer, Amir, Elbaz-Greener, Raccah) Hebrew University of Jerusalem, Israel; Division of Clinical Pharmacy, Institute for Drug Research, School of Pharmacy, Faculty of Medicine (Yanko, Matok, Zmiro, Rotshild, Raccah), Hebrew University of Jerusalem, Israel; Braun School of Public Health and Department of Hematology, Faculty of Medicine (Paltiel), Hebrew University of Jerusalem, Israel
CMAJ. 2023 Jun 19;195(24):E833-E843. doi: 10.1503/cmaj.220960.
Therapeutic options for intermediate- or high-risk pulmonary embolism (PE) include anticoagulation, systemic thrombolysis and catheter-directed thrombolysis (CDT); however, the role of CDT remains controversial. We sought to compare the efficacy and safety of CDT with other therapeutic options using network meta-analysis.
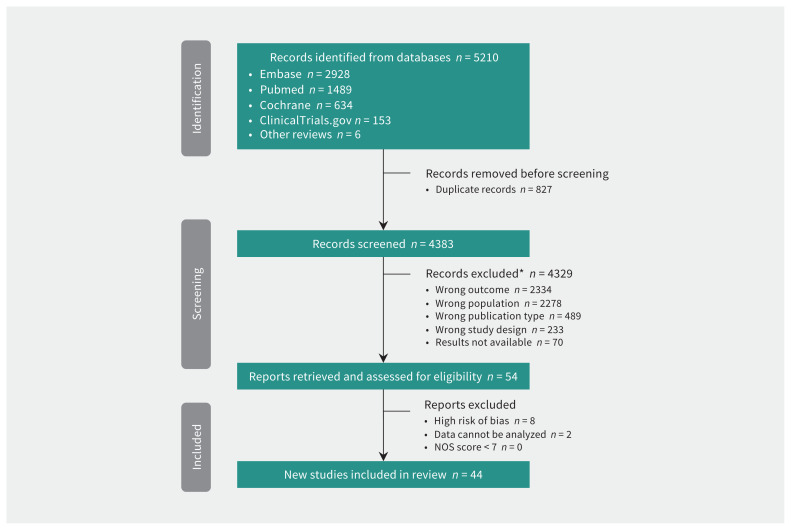
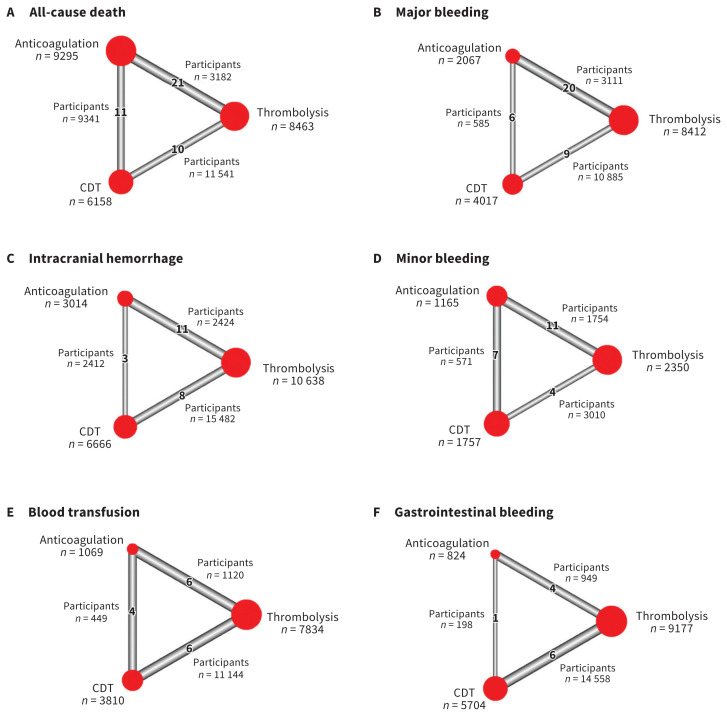
We searched PubMed (MEDLINE), Embase, ClinicalTrials.gov and Cochrane Library from inception to Oct. 18, 2022. We included randomized controlled trials and observational studies that compared therapeutic options for PE, including anticoagulation, systemic thrombolysis and CDT among patients with intermediate- or high-risk PE. The efficacy outcome was in-hospital death. Safety outcomes included major bleeding, intracerebral hemorrhage and minor bleeding.
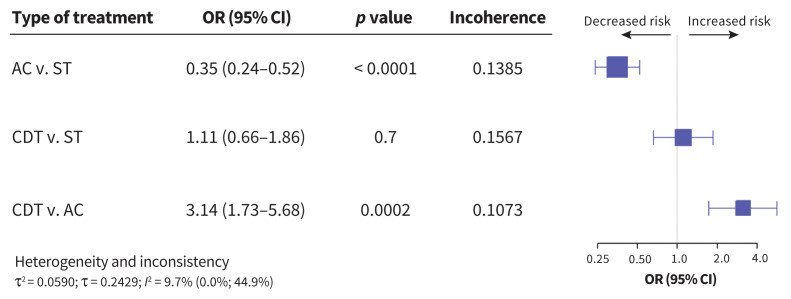
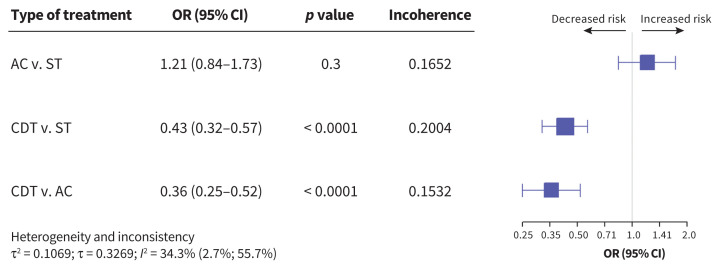
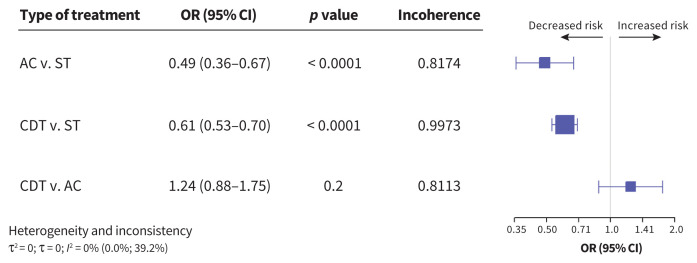
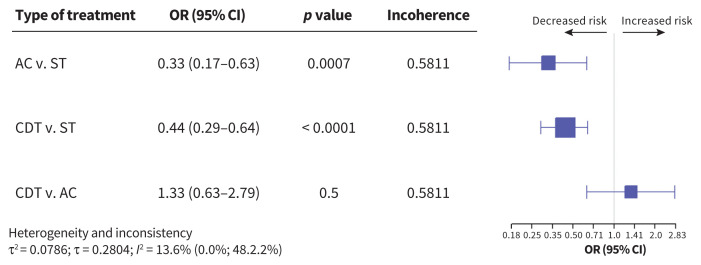
We included data from 44 studies, representing 20 006 patients. Compared with systemic thrombolysis, CDT was associated with a decreased risk of death (odd ratio [OR] 0.43, 95% confidence interval [CI] 0.32-0.57), intracerebral hemorrhage (OR 0.44, 95% CI 0.29-0.64), major bleeding (OR 0.61, 95% CI 0.53-0.70) and blood transfusion (OR 0.46, 95% CI 0.28-0.77). However, no difference in minor bleeding was observed between the 2 therapeutic options (OR 1.11, 95% CI 0.66-1.87). Compared with anticoagulation, CDT was also associated with decreased risk of death (OR 0.36, 95% CI 0.25-0.52), with no increased risk of intracerebral hemorrhage (OR 1.33, 95% CI 0.63-2.79) or major bleeding (OR 1.24, 95% CI 0.88-1.75).
With moderate certainty of evidence, the risk of death and major bleeding complications was lower with CDT than with systemic thrombolysis. Compared with anticoagulation, CDT was associated with a probable lower risk of death and a similar risk of intracerebral hemorrhage, with moderate certainty of evidence. Although these findings are largely based on observational data, CDT may be considered as a first-line therapy in patients with intermediate- or high-risk PE.
PROSPERO - CRD42020182163.
中高危肺栓塞(PE)的治疗选择包括抗凝、全身溶栓和导管定向溶栓(CDT);然而,CDT 的作用仍存在争议。我们旨在通过网络荟萃分析比较 CDT 与其他治疗选择的疗效和安全性。
我们从建库到 2022 年 10 月 18 日在 PubMed(MEDLINE)、Embase、ClinicalTrials.gov 和 Cochrane Library 中进行了检索。我们纳入了比较中高危 PE 患者抗凝、全身溶栓和 CDT 等治疗选择的随机对照试验和观察性研究。疗效结局为院内死亡。安全性结局包括大出血、颅内出血和小出血。
我们纳入了 44 项研究的数据,共代表 20006 例患者。与全身溶栓相比,CDT 降低了死亡风险(比值比 [OR] 0.43,95%置信区间 [CI] 0.32-0.57)、颅内出血风险(OR 0.44,95%CI 0.29-0.64)、大出血风险(OR 0.61,95%CI 0.53-0.70)和输血需求(OR 0.46,95%CI 0.28-0.77)。然而,两种治疗方法之间的小出血发生率无差异(OR 1.11,95%CI 0.66-1.87)。与抗凝相比,CDT 也降低了死亡风险(OR 0.36,95%CI 0.25-0.52),颅内出血风险无增加(OR 1.33,95%CI 0.63-2.79)或大出血风险(OR 1.24,95%CI 0.88-1.75)。
基于中等确定性证据,与全身溶栓相比,CDT 降低了死亡和大出血并发症的风险。与抗凝相比,基于中等确定性证据,CDT 与较低的死亡风险相关,与颅内出血风险相似。尽管这些发现主要基于观察性数据,但 CDT 可被视为中高危 PE 患者的一线治疗方法。
PROSPERO-CRD42020182163。