Oncology Unit, ASST Bergamo ovest, Treviglio (BG), 24047, Italy.
Clinica Oncologica e Centro Regionale di Genetica Oncologica, Università Politecnica delle Marche, Azienda Ospedaliero-Universitaria delle Marche, Via Conca 71, Ancona, 60126, Italy.
BMC Gastroenterol. 2023 Jun 19;23(1):212. doi: 10.1186/s12876-023-02853-w.
In metastatic pancreatic ductal adenocarcinoma (mPDAC), first line treatment options usually include combination regimens of folinic acid, 5-fluorouracil (5-FU), irinotecan, and oxaliplatin (FOLFIRINOX or mFOLFIRINOX) or gemcitabine based regimens such as in combination with albumin-bound paclitaxel (GEM + nab-PTX). After progression, multiple regimens including NALIRI + 5-FU and folinic acid, FOLFIRINOX, 5-FU-based oxaliplatin doublets (OFF, FOLFOX, or XELOX), or 5-FU-based monotherapy (FL, capecitabine, or S-1) are considered appropriate by major guidelines. This network meta-analysis (NMA) aimed to compare the efficacy of different treatment strategies tested as second-line regimens for patients with mPDAC after first-line gemcitabine-based systemic treatment.
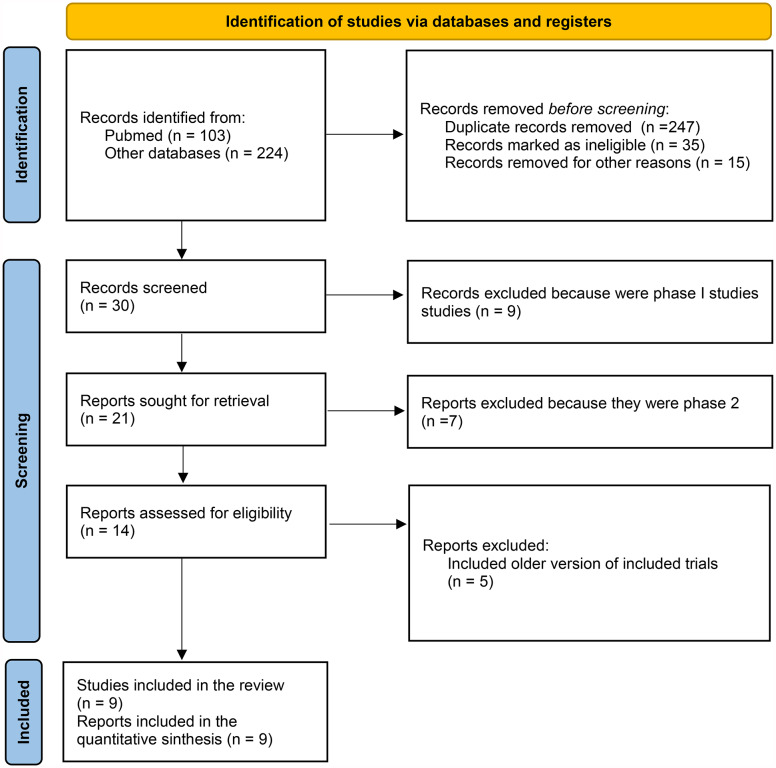
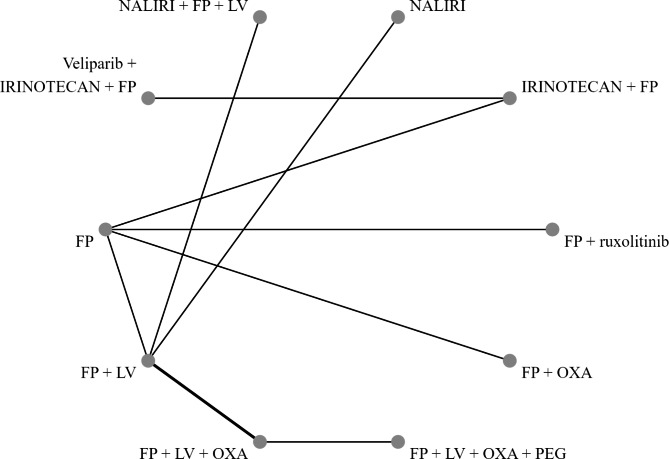
Randomized phase II and III clinical trials (RCTs) were included if they were published or presented in English. Trials of interest compared two active systemic treatments as second-line regimens until disease progression or unacceptable toxicity. We performed a Bayesian NMA with published hazard ratios (HRs) and 95%confidence intervals (CIs) to evaluate the comparative effectiveness of different second-line therapies for mPDAC. The main outcomes of interest were overall survival (OS) and progression free survival (PFS), secondary endpoints were grade 3-4 toxicities. We calculated the relative ranking of agents for each outcome as their surface under the cumulative ranking (SUCRA). A higher SUCRA score meant a higher ranking for efficacy outcomes.
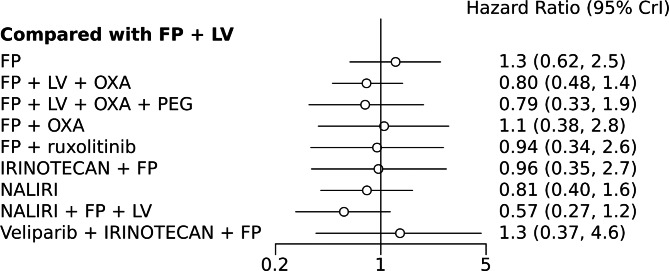
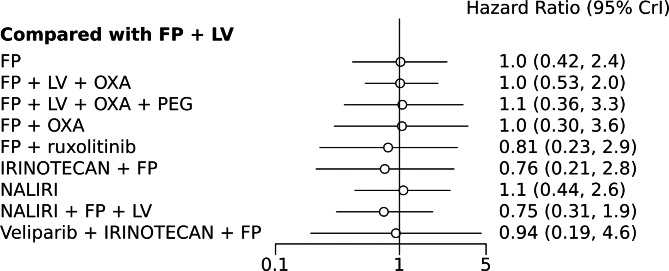
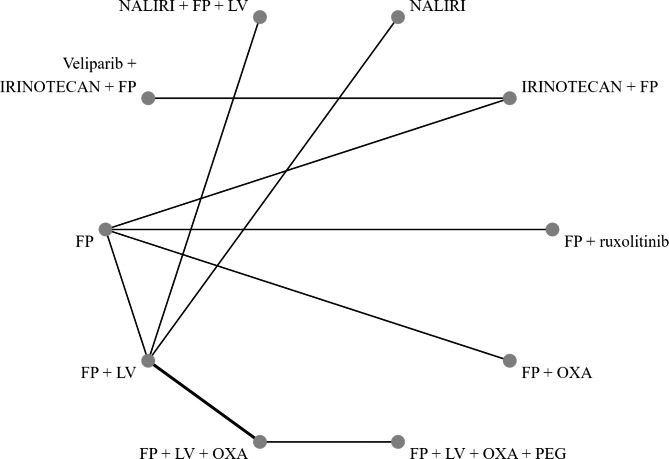
A NMA of 9 treatments was performed for OS (n = 2521 patients enrolled). Compared with 5-FU + folinic acid both irinotecan or NALIRI + fluoropyrimidines had a trend to better OS (HR = 0.76, 95%CI 0.21-2.75 and HR = 0.74, 95%CI 0.31-1.85). Fluoropyrimidines + folinic acid + oxaliplatin were no better than the combination without oxaliplatin. The analysis of treatment ranking showed that the combination of NALIRI + 5-FU + folinic acid was most likely to yield the highest OS results (SUCRA = 0.7). Furthermore, the NMA results indicated that with the highest SUCRA score (SUCRA = 0.91), NALIRI + 5-FU + folinic acid may be the optimal choice for improved PFS amongst all regimens studied.
According to the NMA results, NALIRI + 5-FU, and folinic acid may represent the best second-line treatment for improved survival outcomes in mPDAC. Further evidence from prospective trials is needed to determine the best treatment option for this group of patients.
在转移性胰腺导管腺癌(mPDAC)中,一线治疗方案通常包括亚叶酸、5-氟尿嘧啶(5-FU)、伊立替康和奥沙利铂(FOLFIRINOX 或 mFOLFIRINOX)的联合方案,或基于吉西他滨的方案,如联合白蛋白结合紫杉醇(GEM+ nab-PTX)。疾病进展后,多项指南认为包括 NALIRI+5-FU 和亚叶酸、FOLFIRINOX、基于氟尿嘧啶的奥沙利铂双联(OFF、FOLFOX 或 XELOX)或基于氟尿嘧啶的单药(FL、卡培他滨或 S-1)在内的多种方案均为合适的二线治疗选择。本网络荟萃分析(NMA)旨在比较在一线基于吉西他滨的系统治疗后,mPDAC 患者二线治疗中不同治疗策略的疗效。
如果研究为发表或呈现在英文中的随机 II 期和 III 期临床试验(RCT),则将其纳入研究。感兴趣的试验比较了两种活性全身治疗方案作为二线治疗,直至疾病进展或不可接受的毒性。我们进行了贝叶斯 NMA,使用发表的风险比(HR)和 95%置信区间(CI)来评估不同二线治疗 mPDAC 的相对有效性。主要观察终点为总生存期(OS)和无进展生存期(PFS),次要终点为 3-4 级毒性。我们计算了每个结局的药物相对排名作为累积排序曲线下面积(SUCRA)。SUCRA 得分越高,表明疗效结果的排名越高。
对 9 种治疗方法进行了 OS 的 NMA(n=2521 名入组患者)。与 5-FU+亚叶酸相比,伊立替康或 NALIRI+氟嘧啶均有改善 OS 的趋势(HR=0.76,95%CI 0.21-2.75 和 HR=0.74,95%CI 0.31-1.85)。氟嘧啶+亚叶酸+奥沙利铂并不优于无奥沙利铂的联合方案。治疗排序分析表明,NALIRI+5-FU+亚叶酸的组合最有可能产生最高的 OS 结果(SUCRA=0.7)。此外,NMA 结果表明,NALIRI+5-FU+亚叶酸的 SUCRA 得分最高(SUCRA=0.91),可能是所有研究方案中改善 PFS 的最佳选择。
根据 NMA 结果,NALIRI+5-FU 和亚叶酸可能是 mPDAC 改善生存结局的最佳二线治疗选择。需要进一步的前瞻性试验证据来确定该患者群体的最佳治疗选择。