Bakar Computational Health Sciences Institute, University of California San Francisco, UCSF Valley Tower, Box 2933 Room 21E, 490 Illinois Street, Floor 2, San Francisco, CA, 94143, USA.
Evidence for Access, Genentech Inc., South San Francisco, CA, USA.
Target Oncol. 2023 Jul;18(4):571-583. doi: 10.1007/s11523-023-00973-7. Epub 2023 Jun 21.
Randomized trials have demonstrated that anaplastic lymphoma kinase (ALK) tyrosine kinase inhibitors (TKIs) can be safe and efficacious treatments for patients with ALK-positive advanced non-small-cell lung cancer (aNSCLC). However, their safety, tolerability, effectiveness, and patterns of use in real-world patients remain understudied.
We sought to assess the overall treatment pattern characteristics, safety, and effectiveness outcomes of real-world patients with ALK-positive aNSCLC receiving ALK TKIs.
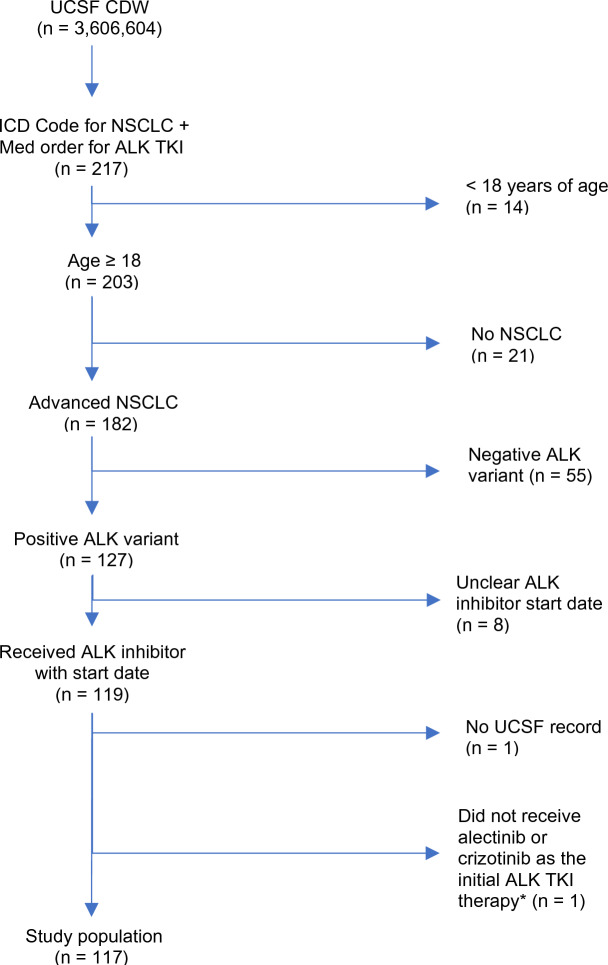
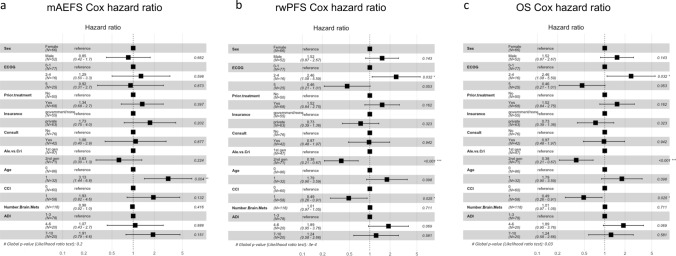
This retrospective cohort study using electronic health record data included adult patients with ALK-positive aNSCLC receiving ALK TKIs between January 2012 and November 2021 at a large tertiary medical center, University of California, San Francisco (UCSF), with alectinib or crizotinib as the initial ALK TKI therapy. Our primary endpoints included the incidence of treatment changes (treatment dose adjustments, interruptions, and discontinuations) during the initial ALK TKI treatment, the count and type of subsequent treatments, rates of serious adverse events (sAEs), and major adverse events (mAEs) leading to any ALK TKI treatment changes. Secondary endpoints included the hazard ratios (HRs) for median mAE-free survival (mAEFS), real-world progression-free survival (rwPFS), and overall survival (OS) when comparing alectinib with crizotinib.
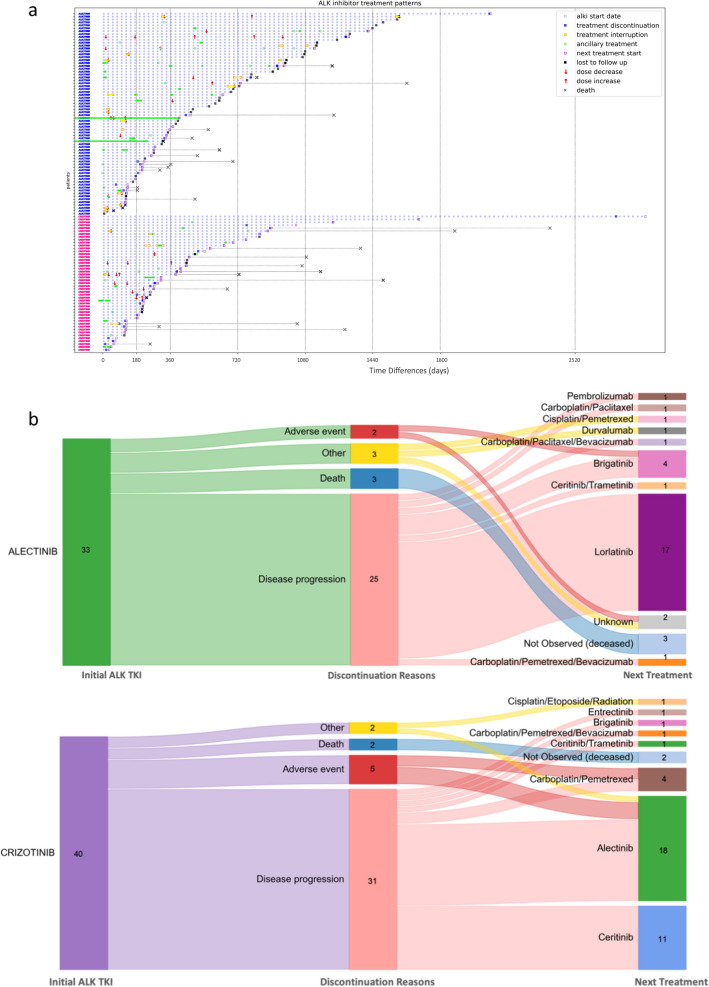
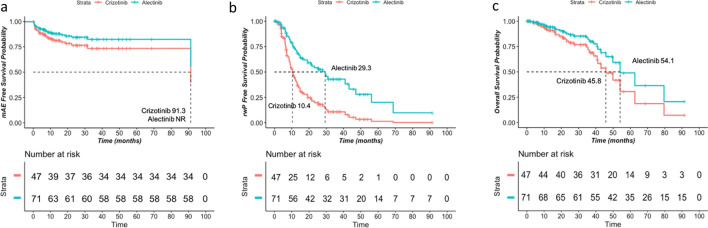
The cohort consisted of 117 adult patients (70 alectinib and 47 crizotinib) with ALK-positive aNSCLC, with 24.8%, 17.9%, and 6.0% experiencing treatment dose adjustments, interruptions, and discontinuation, respectively. Of the 73 patients whose ALK TKI treatments were discontinued, 68 received subsequent treatments including newer generations of ALK TKIs, immune checkpoint inhibitors, and chemotherapies. The most common mAEs were rash (9.9%) and bradycardia (7.0%) for alectinib and liver toxicity (19.1%) for crizotinib. The most common sAEs were pericardial effusion (5.6%) and pleural effusion (5.6%) for alectinib and pulmonary embolism (6.4%) for crizotinib. Patients receiving alectinib versus crizotinib as their first ALK TKI treatment experienced significantly prolonged median rwPFS (29.3 versus 10.4 months) with an HR of 0.38 (95% CI 0.21-0.67), while prolonged median mAEFS (not reached versus 91.3 months) and OS (54.1 versus 45.8 months) were observed in patients receiving alectinib versus crizotinib but did not reach statistical significance. Yet, it is worth noting that there was a high degree of cross-over post-progression, which could significantly confound the overall survival measures.
We found that ALK TKIs were highly tolerable, and alectinib was associated with favorable survival outcomes with longer time to adverse events (AE) requiring medical interventions, disease progression, and death, in the context of real-world use. Proactive monitoring for adverse events such as rash, bradycardia, and hepatotoxicity may help further promote the safe and optimal use of ALK TKIs in the treatment of patients with aNSCLC.
随机试验已经证明,间变性淋巴瘤激酶(ALK)酪氨酸激酶抑制剂(TKI)可作为 ALK 阳性晚期非小细胞肺癌(aNSCLC)患者的安全有效的治疗方法。然而,其在真实世界患者中的安全性、耐受性、有效性和使用模式仍有待研究。
我们旨在评估接受 ALK TKI 治疗的 ALK 阳性 aNSCLC 真实世界患者的总体治疗模式特征、安全性和有效性结局。
这项使用电子健康记录数据的回顾性队列研究纳入了 2012 年 1 月至 2021 年 11 月期间在加州大学旧金山分校(UCSF)接受 ALK TKI 治疗的接受 ALK TKI 治疗的 ALK 阳性 aNSCLC 成年患者,ALK TKI 治疗的初始治疗药物为阿来替尼或克唑替尼。我们的主要终点包括在初始 ALK TKI 治疗期间治疗改变(治疗剂量调整、中断和停药)的发生率、随后治疗的次数和类型、严重不良事件(SAE)的发生率以及导致任何 ALK TKI 治疗改变的主要不良事件(MAE)。次要终点包括比较阿来替尼与克唑替尼时,中位 MAE 无进展生存期(mAEFS)、真实世界无进展生存期(rwPFS)和总生存期(OS)的风险比(HR)。
该队列包括 117 名接受 ALK 阳性 aNSCLC 治疗的成年患者(70 名接受阿来替尼治疗,47 名接受克唑替尼治疗),分别有 24.8%、17.9%和 6.0%的患者经历了治疗剂量调整、中断和停药。在 73 名 ALK TKI 治疗停药的患者中,有 68 名患者接受了后续治疗,包括新一代 ALK TKI、免疫检查点抑制剂和化疗。最常见的 MAE 是皮疹(9.9%)和心动过缓(7.0%)(用于阿来替尼)和肝毒性(19.1%)(用于克唑替尼)。最常见的 SAE 是心包积液(5.6%)和胸腔积液(5.6%)(用于阿来替尼)和肺栓塞(6.4%)(用于克唑替尼)。作为其首种 ALK TKI 治疗药物接受阿来替尼治疗的患者与接受克唑替尼治疗的患者相比,中位 rwPFS 显著延长(29.3 个月与 10.4 个月),HR 为 0.38(95%CI 0.21-0.67),而接受阿来替尼治疗的患者中位 mAEFS (未达到)和 OS(54.1 个月)也明显延长,但与接受克唑替尼治疗的患者相比无统计学意义。然而,值得注意的是,在疾病进展后存在高度的交叉,这可能会严重混淆整体生存措施。
我们发现,ALK TKI 具有高度的耐受性,阿来替尼在真实世界的使用中与更长的时间至需要医疗干预的不良事件(AE)、疾病进展和死亡相关,具有更好的生存结局。对皮疹、心动过缓和肝毒性等不良事件进行积极监测,可能有助于进一步促进 ALK TKI 在治疗 NSCLC 患者中的安全和优化使用。