Department of Thoracic Surgery, The First Affiliated Hospital of Ningbo University, 315010, Ningbo, China.
BMC Pulm Med. 2023 Jun 22;23(1):223. doi: 10.1186/s12890-023-02512-6.
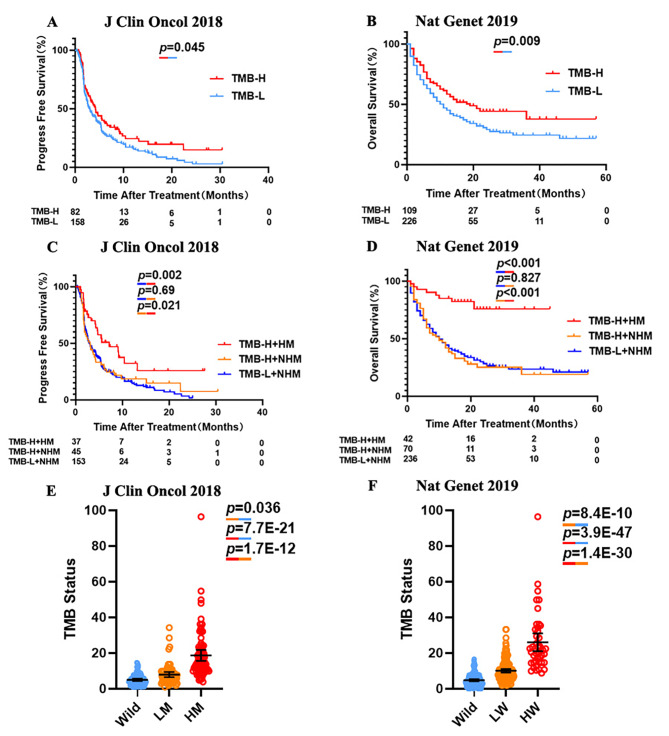
There is an unmet need to identify novel predictive biomarkers that enable more accurate identification of individuals who can benefit from immune checkpoint inhibitor (ICI) therapy. The US FDA recently approved tumor mutational burden (TMB) score of ≥ 10 mut/Mb as a threshold for pembrolizumab treatment of solid tumors. Our study aimed to test the hypothesis that specific gene mutation signature may predict the efficacy of ICI therapy more precisely than high TMB (≥ 10).
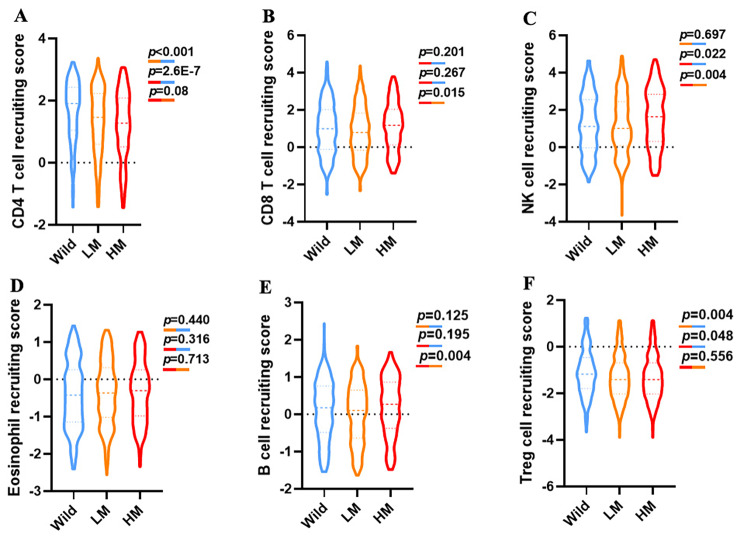
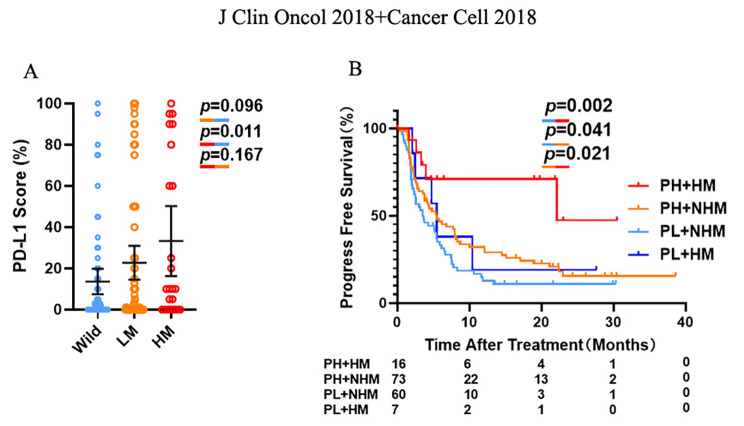
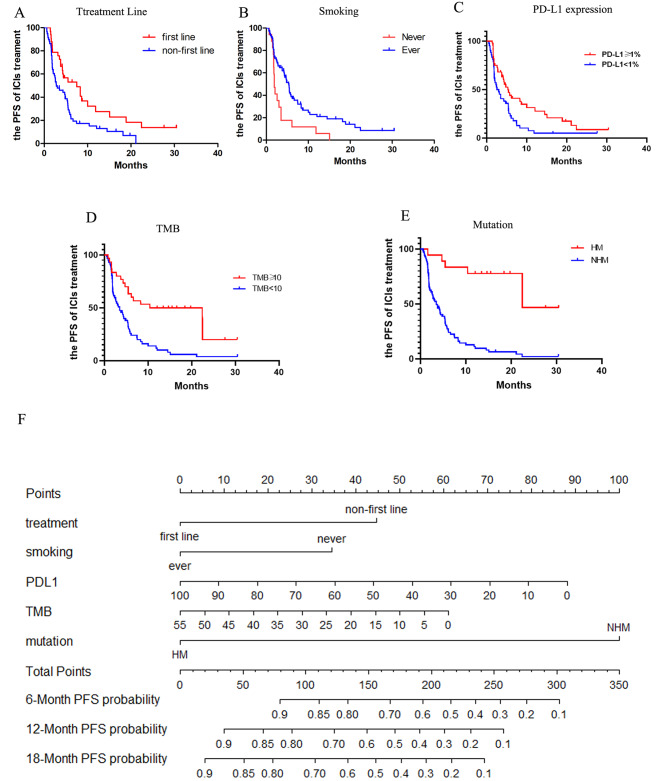
We selected 20 candidate genes that may predict for the efficacy of ICI therapy by the analysis of data from a published cohort of 350 advanced non-small cell lung cancer (NSCLC) patients. Then, we compared the influences of various gene mutation signatures on the efficacy of ICI treatment. They were also compared with PD-L1 and TMB. The Kaplan-Meier method was utilized to evaluate the prognosis univariates, while selected univariates were adopted to develop a systematic nomogram.
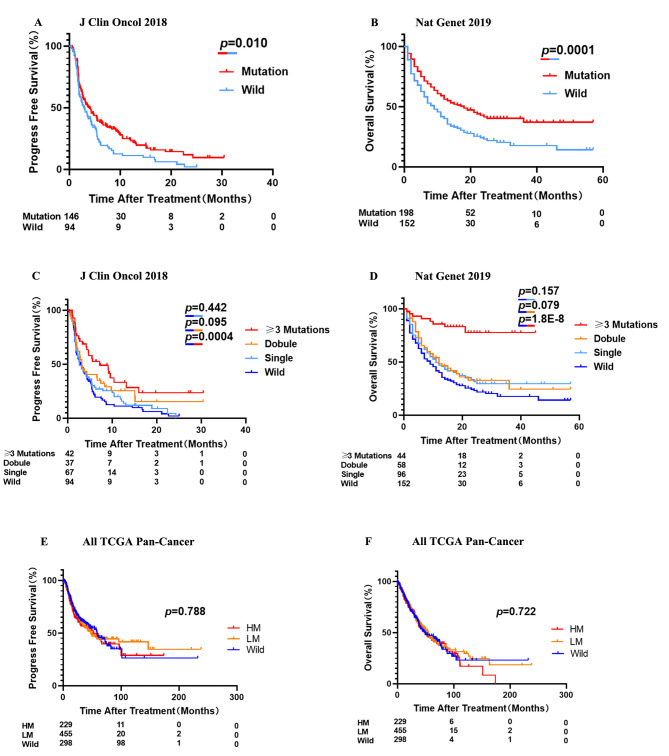
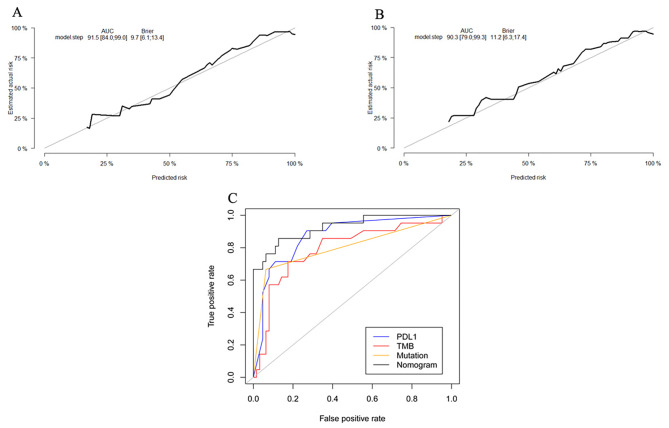
A high mutation signature, where three or more of the 20 selected genes were mutated, was associated with the significant benefits of ICI therapy. Specifically, patients with high mutation signature were confirmed to have better prognosis for ICI treatment, compared with those with wild type (the median PFS: 7.17 vs. 2.90 months, p = 0.0004, HR = 0.47 (95% [CI]:0.32-0.68); the median OS: unreached vs. 9 months, p = 1.8E-8, HR = 0.17 (95% [CI]:0.11-0.25)). Moreover, those patients with the high mutation signature achieved significant ICI treatment benefits, while there was no difference of OS and PFS between patients without the signature but TMB-H (≥ 10) and those without the signature and low TMB(< 10). Finally, we constructed a novel nomogram to evaluate the efficacy of ICI therapy.
A high mutational signature with 3 or more of the 20-gene panel could provide more accurate predictions for the outcomes of ICI therapy than TMB ≥ 10 in NSCLC patients.
目前需要识别新的预测生物标志物,以便更准确地识别出能从免疫检查点抑制剂(ICI)治疗中获益的个体。美国 FDA 最近批准肿瘤突变负荷(TMB)≥10 个突变/Mb 作为帕博利珠单抗治疗实体瘤的阈值。我们的研究旨在检验这样一个假设,即特定的基因突变特征可能比高 TMB(≥10)更能准确预测 ICI 治疗的疗效。
我们通过分析已发表的 350 例晚期非小细胞肺癌(NSCLC)患者队列的数据,选择了 20 个可能预测 ICI 治疗疗效的候选基因。然后,我们比较了各种基因突变特征对 ICI 治疗效果的影响,并与 PD-L1 和 TMB 进行了比较。Kaplan-Meier 法用于评估单变量预后,同时采用单变量选择建立系统列线图。
三个或更多 20 个选定基因发生突变的高突变特征与 ICI 治疗的显著获益相关。具体来说,与野生型相比,具有高突变特征的患者接受 ICI 治疗的预后更好(中位无进展生存期:7.17 与 2.90 个月,p=0.0004,HR=0.47(95%[CI]:0.32-0.68);中位总生存期:未达到与 9 个月,p=1.8E-8,HR=0.17(95%[CI]:0.11-0.25))。此外,那些具有高突变特征的患者确实从 ICI 治疗中获益,而那些没有该特征但 TMB-H(≥10)的患者与那些没有该特征且 TMB 低(<10)的患者之间的 OS 和 PFS 没有差异。最后,我们构建了一个新的列线图来评估 ICI 治疗的疗效。
与 TMB≥10 相比,20 个基因panel 中 3 个或更多基因突变特征可为 NSCLC 患者的 ICI 治疗结果提供更准确的预测。