Fred Hutchinson Cancer Center, Seattle, WA, USA; Department of Pediatrics, University of Washington, Seattle, WA, USA.
Division of Biostatistics, Medical College of Wisconsin, WI, USA; Center for International Blood and Marrow Transplant Research, Milwaukee, WI, USA.
Lancet. 2023 Jul 8;402(10396):129-140. doi: 10.1016/S0140-6736(23)00731-6. Epub 2023 Jun 20.
Severe combined immunodeficiency (SCID) is fatal unless durable adaptive immunity is established, most commonly through allogeneic haematopoietic cell transplantation (HCT). The Primary Immune Deficiency Treatment Consortium (PIDTC) explored factors affecting the survival of individuals with SCID over almost four decades, focusing on the effects of population-based newborn screening for SCID that was initiated in 2008 and expanded during 2010-18.
We analysed transplantation-related data from children with SCID treated at 34 PIDTC sites in the USA and Canada, using the calendar time intervals 1982-89, 1990-99, 2000-09, and 2010-18. Categorical variables were compared by χ test and continuous outcomes by the Kruskal-Wallis test. Overall survival was estimated by the Kaplan-Meier method. A multivariable analysis using Cox proportional hazards regression models examined risk factors for HCT outcomes, including the variables of time interval of HCT, infection status and age at HCT, trigger for diagnosis, SCID type and genotype, race and ethnicity of the patient, non-HLA-matched sibling donor type, graft type, GVHD prophylaxis, and conditioning intensity.
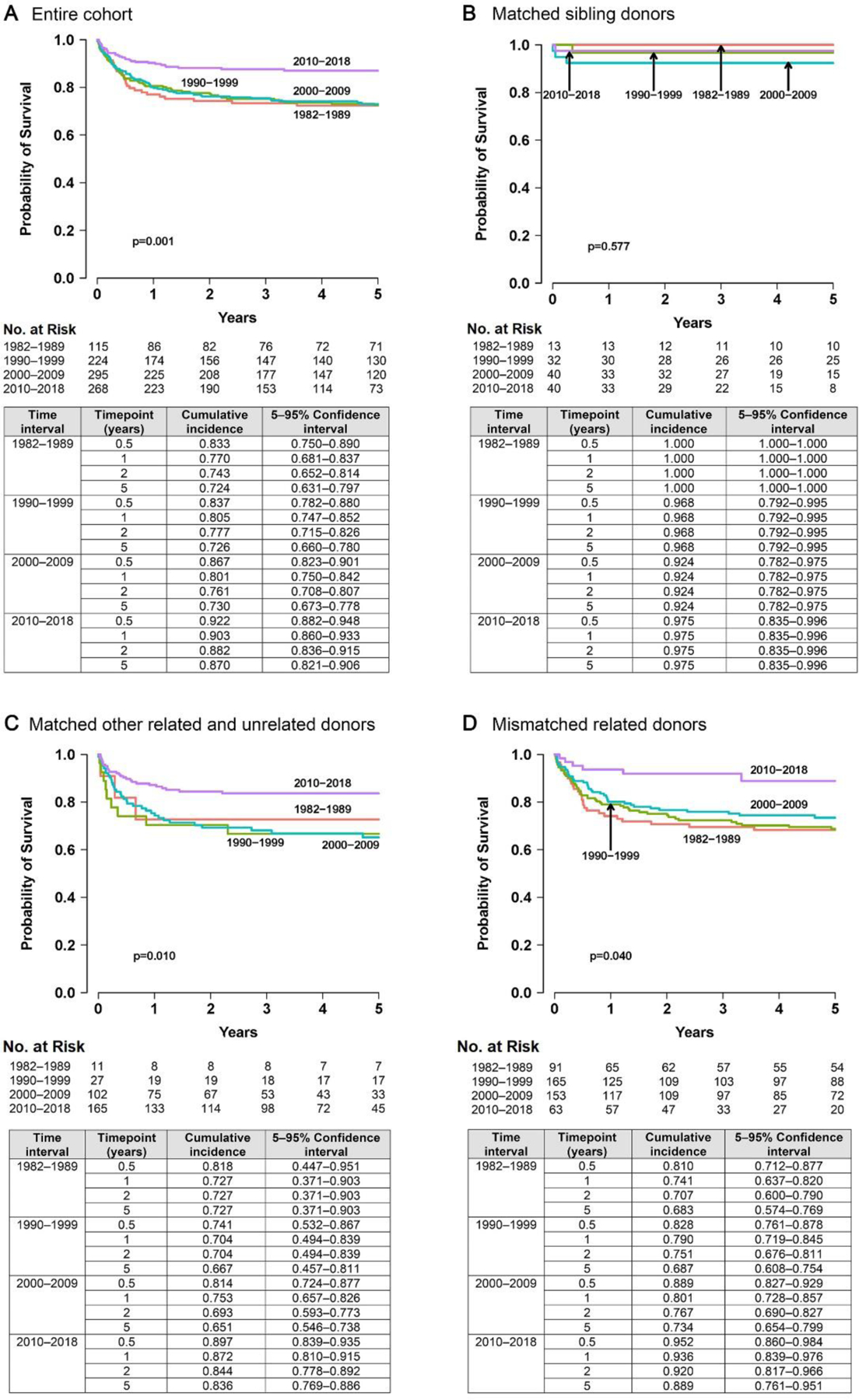
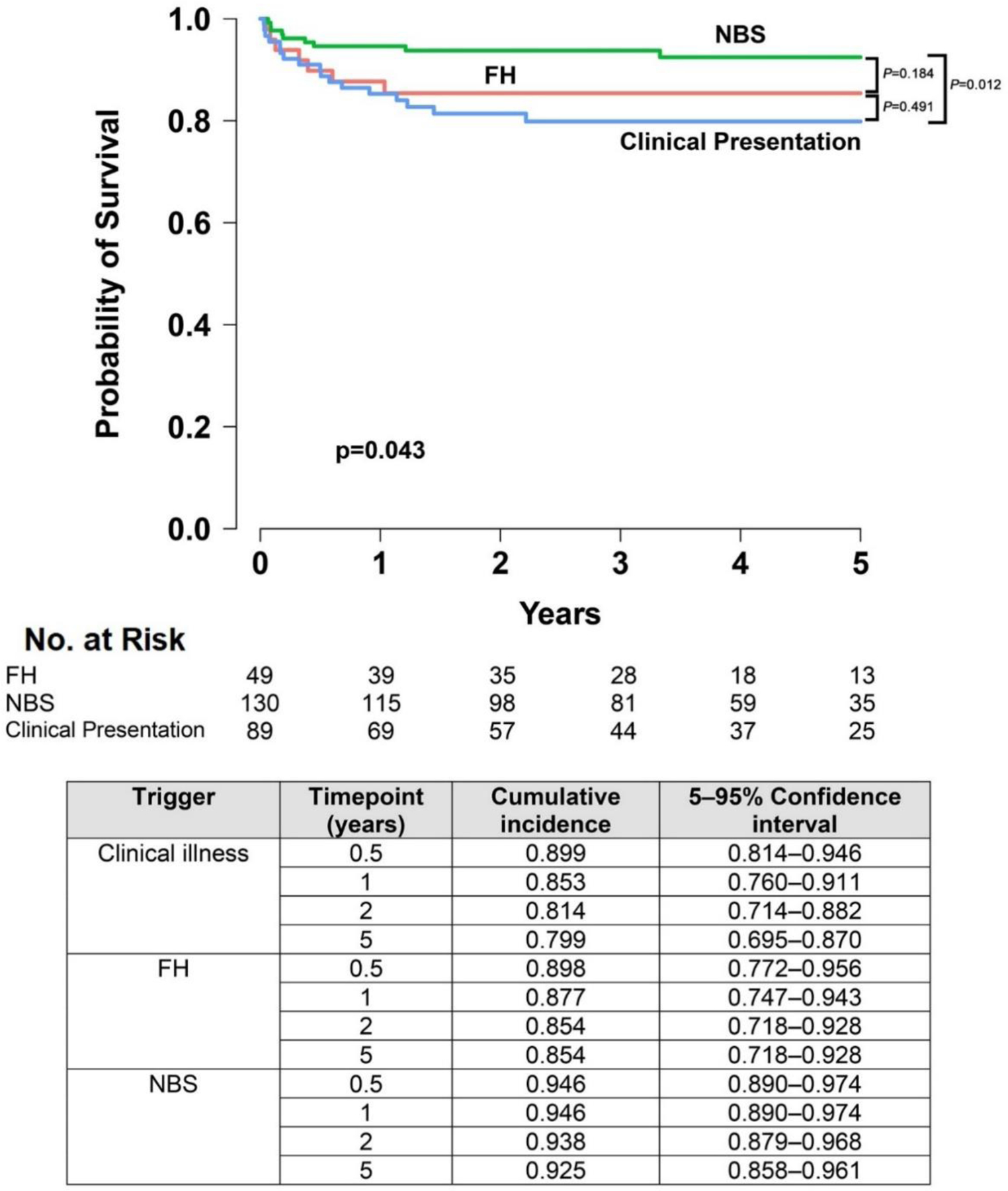
For 902 children with confirmed SCID, 5-year overall survival remained unchanged at 72%-73% for 28 years until 2010-18, when it increased to 87% (95% CI 82·1-90·6; n=268; p=0·0005). For children identified as having SCID by newborn screening since 2010, 5-year overall survival was 92·5% (95% CI 85·8-96·1), better than that of children identified by clinical illness or family history in the same interval (79·9% [69·5-87·0] and 85·4% [71·8-92·8], respectively [p=0·043]). Multivariable analysis demonstrated that the factors of active infection (hazard ratio [HR] 2·41, 95% CI 1·56-3·72; p<0·0001), age 3·5 months or older at HCT (2·12, 1·38-3·24; p=0·001), Black or African-American race (2·33, 1·56-3·46; p<0·0001), and certain SCID genotypes to be associated with lower overall survival during all time intervals. Moreover, after adjusting for several factors in this multivariable analysis, HCT after 2010 no longer conveyed a survival advantage over earlier time intervals studied (HR 0·73, 95% CI 0·43-1·26; p=0·097). This indicated that younger age and freedom from infections at HCT, both directly driven by newborn screening, were the main drivers for recent improvement in overall survival.
Population-based newborn screening has facilitated the identification of infants with SCID early in life, in turn leading to prompt HCT while avoiding infections. Public health programmes worldwide can benefit from this definitive demonstration of the value of newborn screening for SCID.
National Institute of Allergy and Infectious Diseases, Office of Rare Diseases Research, and National Center for Advancing Translational Sciences.
严重联合免疫缺陷(SCID)是致命的,除非建立持久的适应性免疫,这通常是通过异基因造血细胞移植(HCT)来实现的。原发性免疫缺陷治疗联盟(PIDTC)在近四十年的时间里研究了影响 SCID 患者生存的因素,重点是 2008 年启动并在 2010-18 年扩大的 SCID 人群新生儿筛查的效果。
我们分析了美国和加拿大 34 个 PIDTC 站点治疗的 SCID 儿童的移植相关数据,使用的日历时间间隔为 1982-89、1990-99、2000-09 和 2010-18。通过卡方检验比较分类变量,通过 Kruskal-Wallis 检验比较连续结果。使用 Kaplan-Meier 方法估计总生存率。使用 Cox 比例风险回归模型进行多变量分析,以检查 HCT 结果的危险因素,包括 HCT 时间间隔、感染状态和 HCT 时的年龄、诊断触发因素、SCID 类型和基因型、患者的种族和民族、非 HLA 匹配的同胞供体类型、移植物类型、GVHD 预防和调理强度等变量。
对于 902 名确诊为 SCID 的儿童,28 年来,5 年总生存率保持不变,在 2010-18 年之前为 72%-73%,之后增加到 87%(95%CI 82·1-90·6;n=268;p=0·0005)。对于自 2010 年以来通过新生儿筛查确定为 SCID 的儿童,5 年总生存率为 92.5%(95%CI 85.8-96.1),优于同一时期通过临床疾病或家族史确定为 SCID 的儿童(分别为 79.9%[69.5-87.0]和 85.4%[71.8-92.8];p=0.043)。多变量分析表明,活跃感染(危险比[HR]2.41,95%CI 1.56-3.72;p<0.0001)、HCT 时年龄 3.5 个月或以上(2.12,1.38-3.24;p=0.001)、黑人和非裔美国人种族(2.33,1.56-3.46;p<0.0001)和某些 SCID 基因型与所有时间间隔的总生存率降低相关。此外,在对多变量分析中的几个因素进行调整后,HCT 在 2010 年后不再比之前研究的时间间隔具有生存优势(HR 0.73,95%CI 0.43-1.26;p=0.097)。这表明,新生儿筛查直接导致的年轻年龄和 HCT 时无感染是最近总生存率提高的主要驱动因素。
人群新生儿筛查有助于在生命早期发现患有 SCID 的婴儿,从而及时进行 HCT,同时避免感染。全世界的公共卫生计划都可以从 SCID 新生儿筛查的价值得到明确证明中受益。
国家过敏和传染病研究所、罕见病研究办公室和国家转化医学推进中心。