Division of Pediatric Allergy, Immunology, and Bone Marrow Transplantation, University of California San Francisco Benioff Children's Hospital, San Francisco, California.
Division of Pediatric Allergy, Immunology, and Bone Marrow Transplantation, University of California San Francisco Benioff Children's Hospital, San Francisco, California; Department of Clinical Pharmacy, University of California San Francisco, San Francisco, California.
Biol Blood Marrow Transplant. 2019 Jul;25(7):1355-1362. doi: 10.1016/j.bbmt.2019.03.008. Epub 2019 Mar 12.
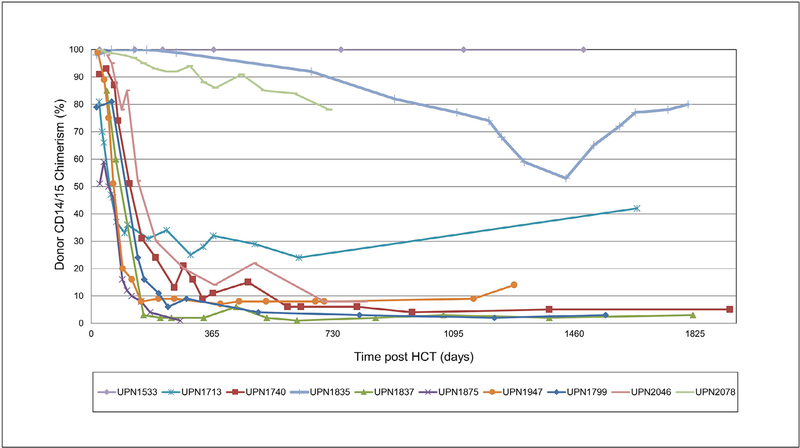
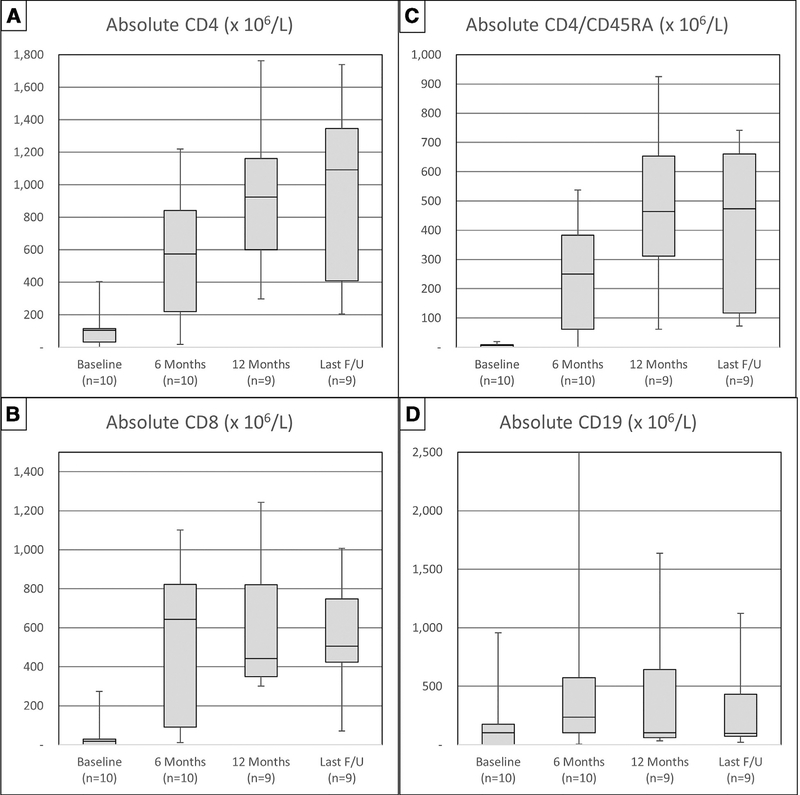
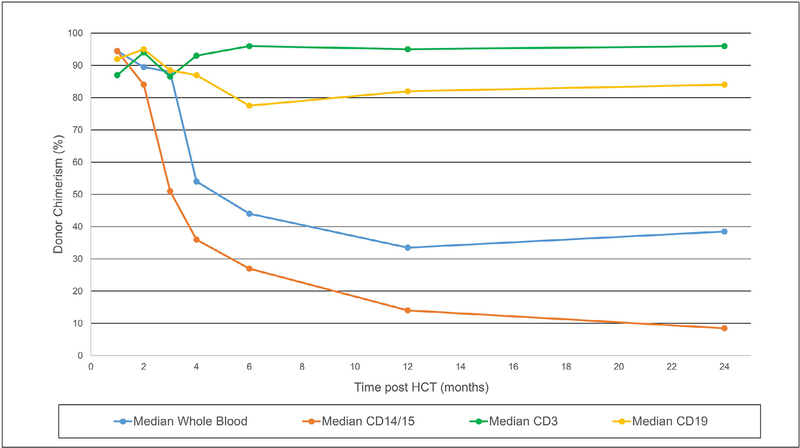
After allogeneic hematopoietic cell transplantation (HCT), the minimal myeloid chimerism required for full T and B cell reconstitution in patients with severe combined immunodeficiency (SCID) is unknown. We retrospectively reviewed our experience with low-exposure busulfan (cumulative area under the curve, 30 mg·hr/L) in 10 SCID patients undergoing either first or repeat HCT from unrelated or haploidentical donors. The median busulfan dose required to achieve this exposure was 5.9 mg/kg (range, 4.8 to 9.1). With a median follow-up of 4.5 years all patients survived, with 1 requiring an additional HCT. Donor myeloid chimerism was generally >90% at 1 month post-HCT, but in most patients it fell during the next 3 months, such that 1-year median myeloid chimerism was 14% (range, 2% to 100%). Six of 10 patients had full T and B cell reconstitution, despite myeloid chimerism as low as 3%. Three patients have not recovered B cell function at over 2 years post-HCT, 2 of them in the setting of treatment with rituximab for post-HCT autoimmunity. Low-exposure busulfan was well tolerated and achieved sufficient myeloid chimerism for full immune reconstitution in over 50% of patients. However, other factors beyond busulfan exposure may also play critical roles in determining long-term myeloid chimerism and full T and B cell reconstitution.
异基因造血细胞移植(HCT)后,严重联合免疫缺陷(SCID)患者完全重建 T 和 B 细胞所需的最小骨髓嵌合状态尚不清楚。我们回顾性分析了 10 例 SCID 患者在接受无关或单倍体供体首次或重复 HCT 时接受低剂量白消安(累积 AUC 为 30mg·hr/L)的经验。达到这种暴露所需的白消安中位剂量为 5.9mg/kg(范围为 4.8 至 9.1)。中位随访 4.5 年后,所有患者均存活,其中 1 例需要额外的 HCT。供者骨髓嵌合状态在 HCT 后 1 个月通常>90%,但在大多数患者中,在接下来的 3 个月内下降,因此 1 年时中位骨髓嵌合率为 14%(范围为 2%至 100%)。尽管骨髓嵌合率低至 3%,但 10 例患者中有 6 例完全重建了 T 和 B 细胞功能。在 HCT 后超过 2 年,有 3 例患者仍未恢复 B 细胞功能,其中 2 例在 HCT 后自身免疫性疾病中接受利妥昔单抗治疗。低剂量白消安耐受性良好,在超过 50%的患者中实现了足够的骨髓嵌合以完全重建免疫。然而,除白消安暴露外,其他因素也可能在确定长期骨髓嵌合状态和完全重建 T 和 B 细胞功能方面发挥关键作用。