Rusch C, Flanagan R, Suh H, Subramanian I
Food Science and Human Nutrition Department, Center for Nutritional Sciences, University of Florida, Gainesville, FL, USA.
Department of Neurology, Norman Fixel Institute for Neurological Diseases, University of Florida, Gainesville, FL, USA.
NPJ Parkinsons Dis. 2023 Jun 24;9(1):98. doi: 10.1038/s41531-023-00541-w.
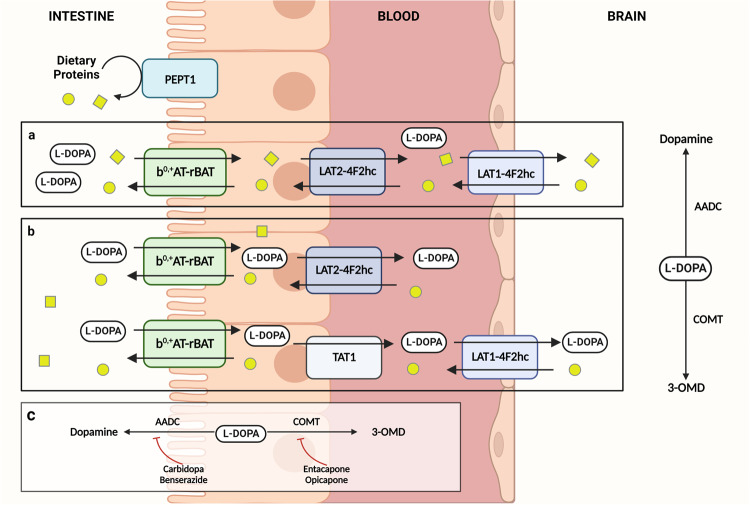
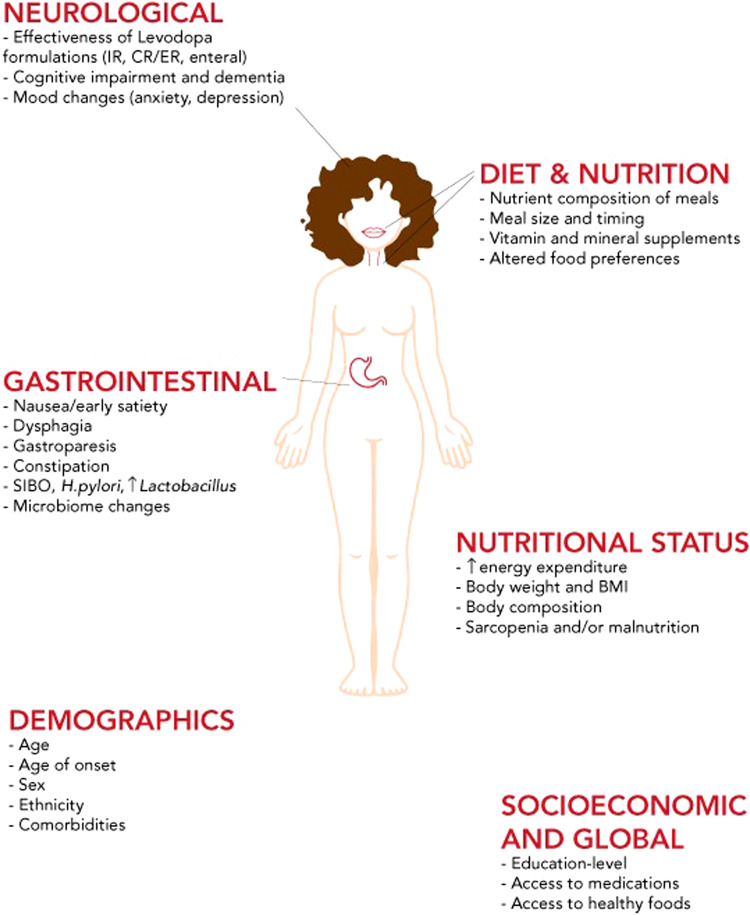
Administration of levodopa for Parkinson's disease (PD) has remained the most effective therapy for symptom management despite being in use for over 50 years. Advancing disease and age, changing tolerability and gastrointestinal (GI) dysfunction may result in change in dietary habits and body weight, as well as unpredictable motor fluctuations and dyskinesias. Dietary proteins which convert into amino acids after digestion are implicated as major factors that inhibit levodopa absorption. For people living with PD (PwP) who experience motor fluctuations, low protein diets (LPD) and protein redistribution diets (PRD) may be effective and are often recommended as a non-pharmacologic approach for improving levodopa bioavailability. However, there is a lack of consensus on a standard definition of these diets and appropriate treatment algorithms for usage. This may be due to the paucity of high-level evidence of LPD and PRD in PwP and whether all or specific subgroups of patients would benefit from these strategies. Managing diet and protein intake with proper education and monitoring may reduce complications associated with these diets such as dyskinesias and unintentional weight loss. Additionally, alterations to medications and GI function may alter levodopa pharmacokinetics. In this narrative review we focus on 1) mechanisms of dietary protein and levodopa absorption in the intestine and blood brain barrier, 2) dietetic approaches to manage protein and levodopa interactions and 3) practical issues for treating PwP as well as future directions to be considered.
尽管左旋多巴已用于治疗帕金森病(PD)50多年,但它仍然是症状管理最有效的疗法。疾病进展、年龄增长、耐受性改变以及胃肠道(GI)功能障碍可能导致饮食习惯和体重变化,以及不可预测的运动波动和异动症。消化后转化为氨基酸的膳食蛋白质被认为是抑制左旋多巴吸收的主要因素。对于经历运动波动的帕金森病患者(PwP),低蛋白饮食(LPD)和蛋白质重新分配饮食(PRD)可能有效,并且通常被推荐作为提高左旋多巴生物利用度的非药物方法。然而,对于这些饮食的标准定义以及合适的使用治疗算法缺乏共识。这可能是由于PwP中LPD和PRD的高级别证据较少,以及所有患者或特定亚组患者是否会从这些策略中获益尚不清楚。通过适当的教育和监测来管理饮食和蛋白质摄入量,可能会减少与这些饮食相关的并发症, 如异动症和意外体重减轻。此外,药物和胃肠功能改变可能会改变左旋多巴的药代动力学。在这篇叙述性综述中,我们重点关注:1)膳食蛋白质和左旋多巴在肠道及血脑屏障中的吸收机制;2)管理蛋白质和左旋多巴相互作用的饮食方法;3)治疗PwP的实际问题以及未来需要考虑的方向。