Singh Kavita, Joshi Awantika, Venkateshmurthy Nikhil Srinivasapura, Rahul Rahul, Huffman Mark D, Tandon Nikhil, Prabhakaran Dorairaj
Public Health Foundation of India, Gurugram, Haryana 122002 India.
Centre for Chronic Disease Control, New Delhi, India.
Glob Implement Res Appl. 2023 Jun 5:1-12. doi: 10.1007/s43477-023-00087-2.
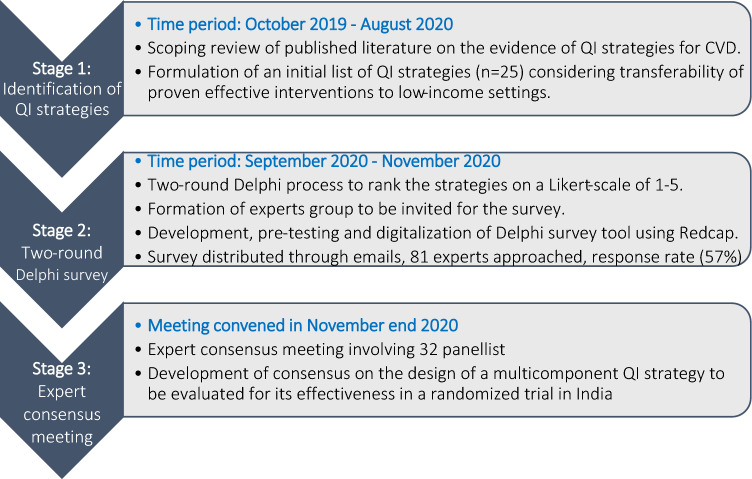
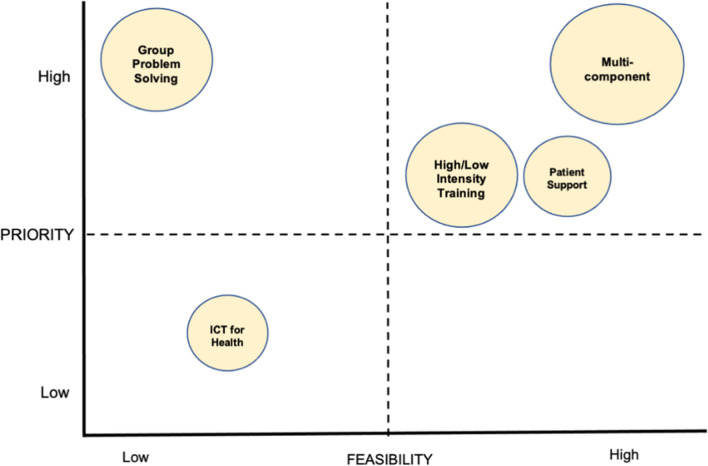
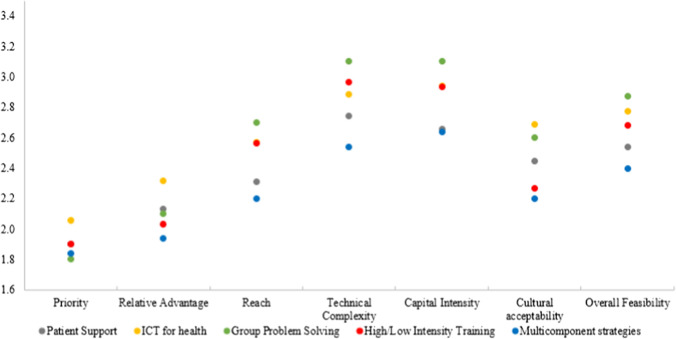
Providing quality cardiovascular disease (CVD) care in low resource setting requires understanding of priority and effective interventions. This study aimed to identify and prioritize evidence-based quality improvement strategies for CVD care in India using a modified two-round Delphi process in which, we asked 46 experts (clinicians, researchers, program implementers and policy makers) to rate 25 proven CVD care strategies grouped into: (1) patient support, (2) information communication technology (ICT) for health, (3) group problem solving, (4) training, and (5) multicomponent strategy on a scale of 1 (highest/best)-5 (lowest/worst) on priority, relative advantage, and feasibility. Subsequently, we convened an expert consensus panel of 32 members to deliberate and achieve consensus regarding the prioritized set of strategies for CVD care. The Delphi study found that group problem solving strategies achieved the best score for priority (1.80) but fared poorly on feasibility (2.88). Compared to others, multicomponent strategies were rated favorably across all domains (priority = 1.84, relative advantage = 1.94, and feasibility = 2.40). The ICT for health strategies achieved the worst scores for priority = 2.01, relative advantage = 2.31, and feasibility = 2.85. Training and patient support strategies scored moderately across all domains. The expert panel narrowed the selection of a multicomponent strategy consisting of (1) electronic health records with clinical decision-support system, (2) non-physician health worker facilitated care, (3) patient education materials, (4) text-message based reminders for healthy lifestyle, and (5) audit and feedback report for providers. Future research will evaluate the real-world feasibility and effectiveness of the multicomponent strategy in patients with CVD in a low- and middle-income country setting.
The online version contains supplementary material available at 10.1007/s43477-023-00087-2.
在资源匮乏的环境中提供高质量的心血管疾病(CVD)护理需要了解优先事项和有效的干预措施。本研究旨在通过改进的两轮德尔菲法确定印度心血管疾病护理基于证据的质量改进策略并对其进行优先排序,在该方法中,我们让46位专家(临床医生、研究人员、项目实施者和政策制定者)对25种已证实的心血管疾病护理策略进行评分,这些策略分为:(1)患者支持,(2)健康信息通信技术(ICT),(3)小组问题解决,(4)培训,以及(5)多组分策略,评分范围为1(最高/最佳)至5(最低/最差),涉及优先性、相对优势和可行性。随后,我们召集了一个由32名成员组成的专家共识小组,就心血管疾病护理的优先策略集进行审议并达成共识。德尔菲研究发现,小组问题解决策略在优先性方面得分最高(1.80),但在可行性方面表现不佳(2.88)。与其他策略相比,多组分策略在所有领域的评分都较高(优先性 = 1.84,相对优势 = 1.94,可行性 = 2.40)。健康信息通信技术策略在优先性方面得分最低,为2.01,相对优势为2.31,可行性为2.85。培训和患者支持策略在所有领域的得分中等。专家小组缩小了对一种多组分策略的选择范围,该策略包括:(1)带有临床决策支持系统的电子健康记录,(2)非医师卫生工作者辅助护理,(3)患者教育材料,(4)基于短信的健康生活方式提醒,以及(5)针对提供者的审核和反馈报告。未来的研究将评估该多组分策略在低收入和中等收入国家环境中心血管疾病患者中的实际可行性和有效性。
在线版本包含可在10.1007/s43477-023-00087-2获取的补充材料。