From the Population Health Research Institute, McMaster University and Hamilton Health Sciences, Hamilton, ON (S.Y., P.J., P. Gao, K.T., C.C., T.M., J.T., J.B.), Queen's University, Kingston, ON (K. Yeates), and Université Laval Institut Universitaire de Cardiologie et de Pneumologie de Québec, Quebec, QC (G.D.) - all in Canada; the University of the Philippines, Manila (A.D.); St. John's Medical College, Bangalore, India (D.X., P. Girish, F.X., P.P.); Fundación Oftalmológica de Santander, Universidad de Santander, Bucaramanga, Colombia (P.L.-J., C.R.); Universiti Teknologi MARA Selayang, Selangor, and UCSI University, Cheras, Kuala Lumpur - both in Malaysia (K. Yusoff); Universitas Indonesia, National Cardiovascular Center, Jakarta (A.S.); Fattouma Bourguiba Hospital and University of Monastir, Monastir, Tunisia (H.G.); and Eminence, Dhaka, Bangladesh (S.T.).
N Engl J Med. 2021 Jan 21;384(3):216-228. doi: 10.1056/NEJMoa2028220. Epub 2020 Nov 13.
A polypill comprising statins, multiple blood-pressure-lowering drugs, and aspirin has been proposed to reduce the risk of cardiovascular disease.
Using a 2-by-2-by-2 factorial design, we randomly assigned participants without cardiovascular disease who had an elevated INTERHEART Risk Score to receive a polypill (containing 40 mg of simvastatin, 100 mg of atenolol, 25 mg of hydrochlorothiazide, and 10 mg of ramipril) or placebo daily, aspirin (75 mg) or placebo daily, and vitamin D or placebo monthly. We report here the outcomes for the polypill alone as compared with matching placebo, for aspirin alone as compared with matching placebo, and for the polypill plus aspirin as compared with double placebo. For the polypill-alone and polypill-plus-aspirin comparisons, the primary outcome was death from cardiovascular causes, myocardial infarction, stroke, resuscitated cardiac arrest, heart failure, or revascularization. For the aspirin comparison, the primary outcome was death from cardiovascular causes, myocardial infarction, or stroke. Safety was also assessed.
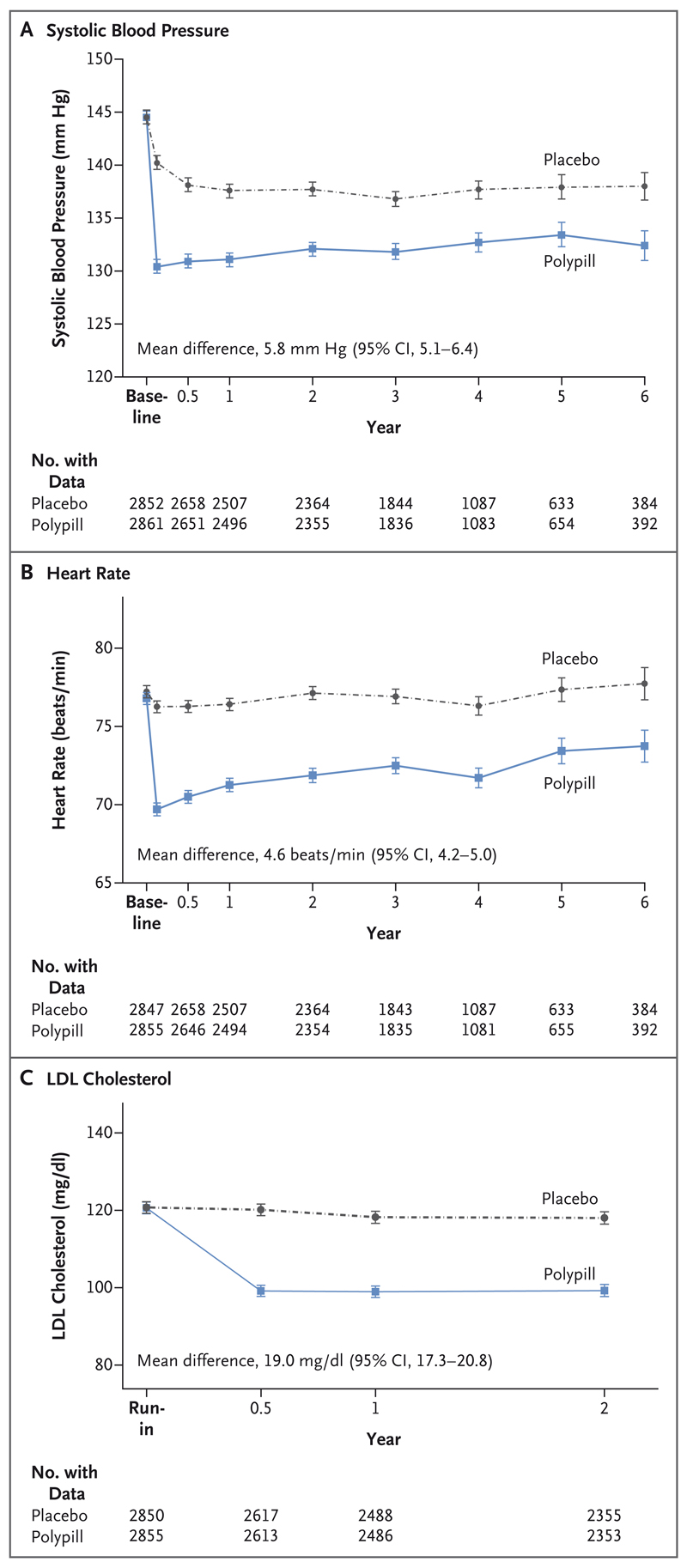
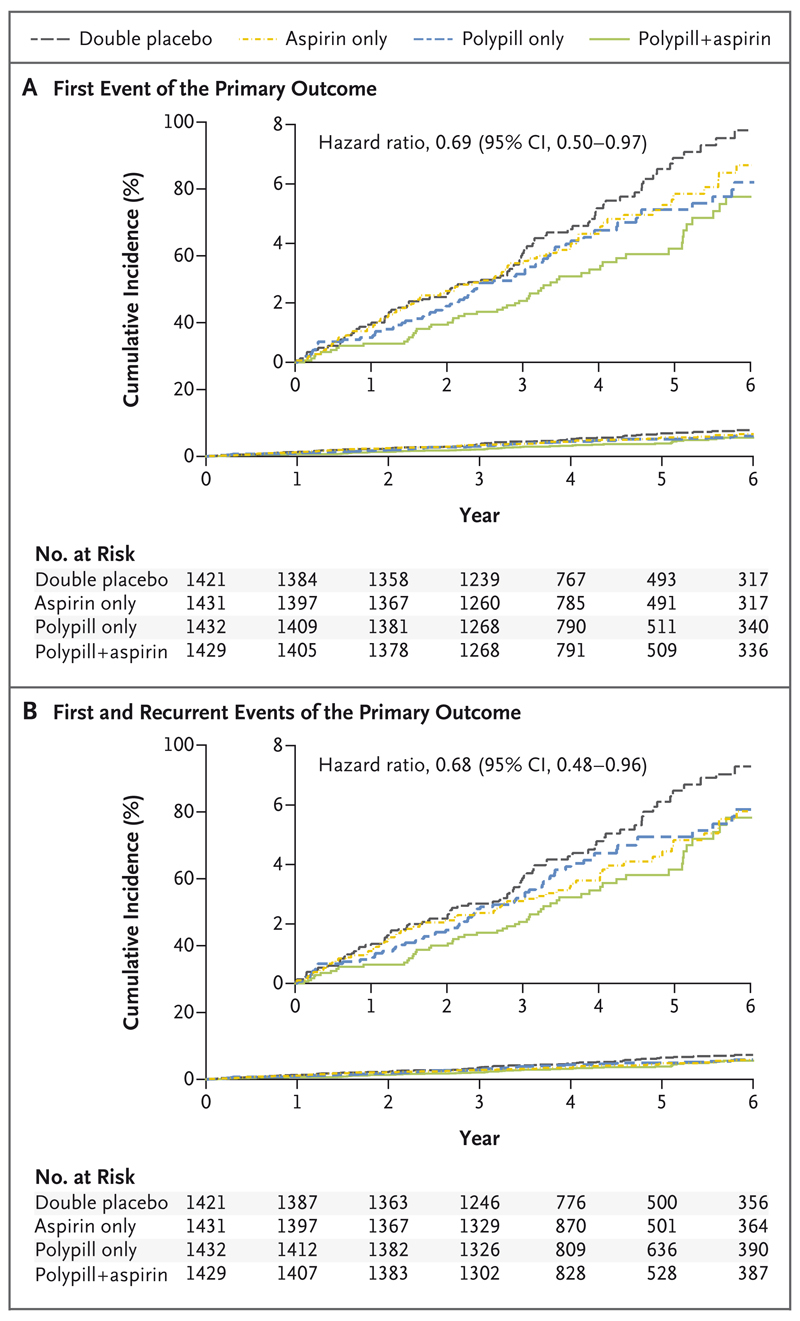
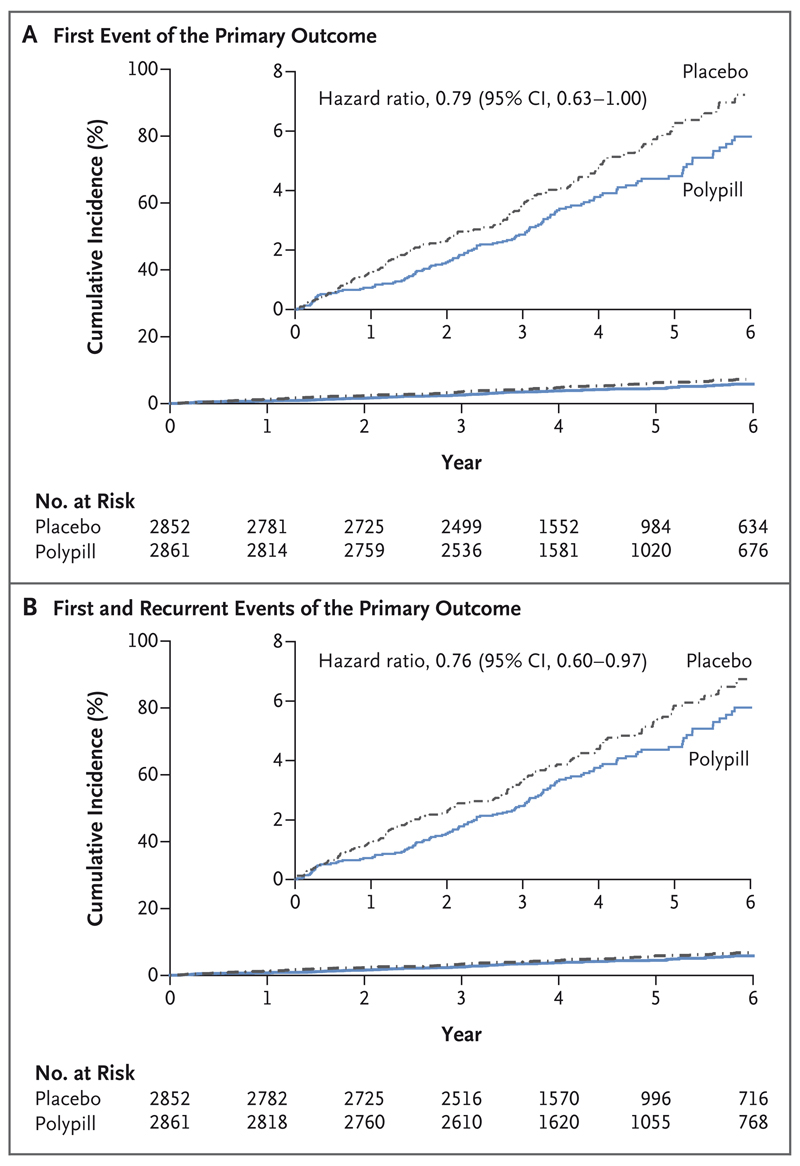
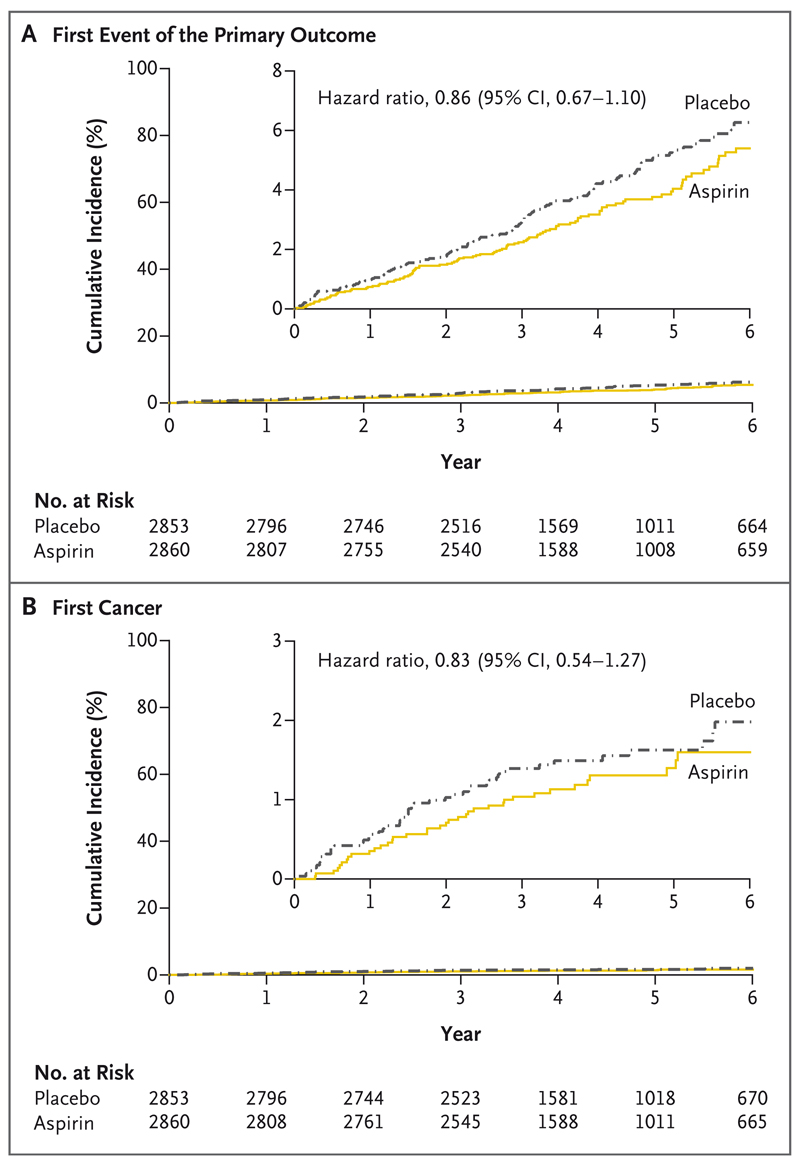
A total of 5713 participants underwent randomization, and the mean follow-up was 4.6 years. The low-density lipoprotein cholesterol level was lower by approximately 19 mg per deciliter and systolic blood pressure was lower by approximately 5.8 mm Hg with the polypill and with combination therapy than with placebo. The primary outcome for the polypill comparison occurred in 126 participants (4.4%) in the polypill group and in 157 (5.5%) in the placebo group (hazard ratio, 0.79; 95% confidence interval [CI], 0.63 to 1.00). The primary outcome for the aspirin comparison occurred in 116 participants (4.1%) in the aspirin group and in 134 (4.7%) in the placebo group (hazard ratio, 0.86; 95% CI, 0.67 to 1.10). The primary outcome for the polypill-plus-aspirin comparison occurred in 59 participants (4.1%) in the combined-treatment group and in 83 (5.8%) in the double-placebo group (hazard ratio, 0.69; 95% CI, 0.50 to 0.97). The incidence of hypotension or dizziness was higher in groups that received the polypill than in their respective placebo groups.
Combined treatment with a polypill plus aspirin led to a lower incidence of cardiovascular events than did placebo among participants without cardiovascular disease who were at intermediate cardiovascular risk. (Funded by the Wellcome Trust and others; TIPS-3 ClinicalTrials.gov number, NCT01646437.).
包含他汀类药物、多种降压药物和阿司匹林的复方药被提议用于降低心血管疾病风险。
我们采用 2×2×2 析因设计,将 INTERHEART 风险评分升高且无心血管疾病的参与者随机分配,每日服用复方药(含 40mg 辛伐他汀、100mg 阿替洛尔、25mg 氢氯噻嗪和 10mg 雷米普利)或安慰剂、每日服用阿司匹林(75mg)或安慰剂、每月服用维生素 D 或安慰剂。我们在此报告单独使用复方药与匹配安慰剂相比、单独使用阿司匹林与匹配安慰剂相比、以及复方药加阿司匹林与双重安慰剂相比的结果。对于复方药单独使用和复方药加阿司匹林使用的比较,主要结局是心血管原因导致的死亡、心肌梗死、卒中和复苏性心脏骤停、心力衰竭或血运重建。对于阿司匹林的比较,主要结局是心血管原因导致的死亡、心肌梗死或卒。也评估了安全性。
共有 5713 名参与者被随机分配,平均随访时间为 4.6 年。与安慰剂相比,服用复方药和联合治疗可使低密度脂蛋白胆固醇水平降低约 19mg/dL,收缩压降低约 5.8mmHg。与安慰剂相比,复方药比较的主要结局发生在 126 名参与者(4.4%)中,而在 157 名参与者(5.5%)中发生在安慰剂组(风险比,0.79;95%置信区间[CI],0.63 至 1.00)。阿司匹林比较的主要结局发生在 116 名参与者(4.1%)中,在阿司匹林组和 134 名参与者(4.7%)中发生在安慰剂组(风险比,0.86;95%CI,0.67 至 1.10)。复方药加阿司匹林联合治疗的主要结局发生在 59 名参与者(4.1%)中,在双重安慰剂组中发生在 83 名参与者(5.8%)(风险比,0.69;95%CI,0.50 至 0.97)。与各自的安慰剂组相比,服用复方药的参与者低血压或头晕的发生率更高。
对于处于中间心血管风险的无心血管疾病参与者,与安慰剂相比,联合使用复方药加阿司匹林治疗可降低心血管事件的发生率。(由威康信托基金会和其他机构资助;TIPS-3 ClinicalTrials.gov 编号,NCT01646437。)