Department of Health Policy and Management, Harvard T.H. Chan School of Public Health, Boston, Massachusetts.
Department of Medicine, Brigham and Women's Hospital, Boston, Massachusetts.
JAMA Netw Open. 2023 Jun 1;6(6):e2320583. doi: 10.1001/jamanetworkopen.2023.20583.
Limiting the use of high-risk medications (HRMs) among older adults is a national priority to provide a high quality of care for older beneficiaries of both Medicare Advantage and traditional fee-for-service Medicare Part D plans.
To evaluate the differences in the rate of HRM prescription fills among beneficiaries of traditional Medicare vs Medicare Advantage Part D plans and to examine the extent to which these differences change over time and the patient-level factors associated with higher rates of HRMs.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study used a 20% sample of Medicare Part D data on filled drug prescriptions from 2013 to 2017 and a 40% sample from 2018. The sample comprised Medicare beneficiaries aged 66 years or older who were enrolled in Medicare Advantage or traditional Medicare Part D plans. Data were analyzed between April 1, 2022, and April 15, 2023.
The primary outcome was the number of unique HRMs prescribed to older Medicare beneficiaries per 1000 beneficiaries. Linear regression models were used to model the primary outcome, adjusting for patient characteristics and county characteristics and including hospital referral region fixed effects.
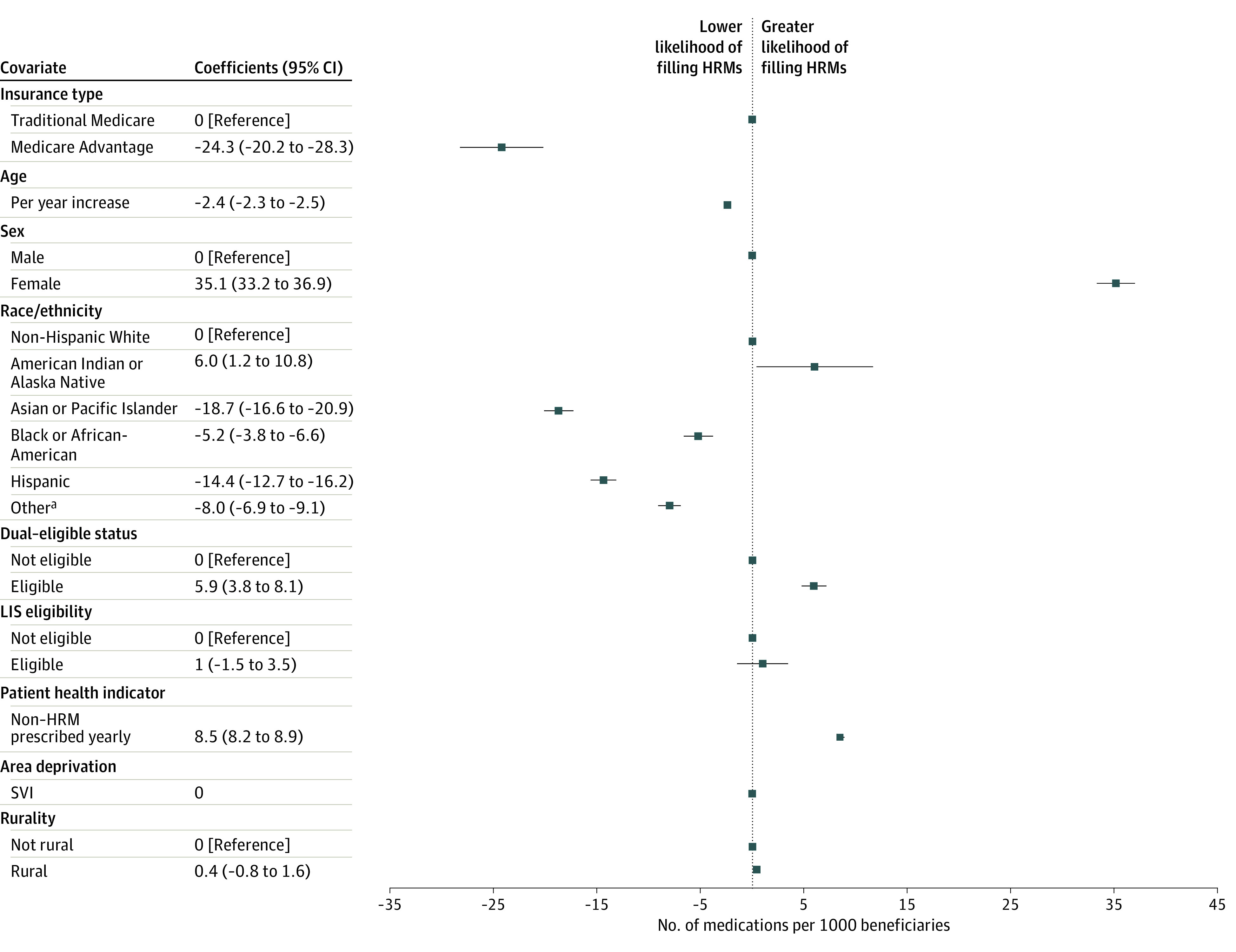
The sample included 5 595 361 unique Medicare Advantage beneficiaries who were propensity score-matched on a year-by-year basis to 6 578 126 unique traditional Medicare beneficiaries between 2013 and 2018, resulting in 13 704 348 matched pairs of beneficiary-years. The traditional Medicare vs Medicare Advantage cohorts were similar in age (mean [SD] age, 75.65 [7.53] years vs 75.60 [7.38] years), proportion of males (8 127 261 [59.3%] vs 8 137 834 [59.4%]; standardized mean difference [SMD] = 0.002), and predominant race and ethnicity (77.1% vs 77.4% non-Hispanic White; SMD = 0.05). On average in 2013, Medicare Advantage beneficiaries filled 135.1 (95% CI, 128.4-142.6) unique HRMs per 1000 beneficiaries compared with 165.6 (95% CI, 158.1-172.3) HRMs per 1000 beneficiaries for traditional Medicare. In 2018, the rate of HRMs had decreased to 41.5 (95% CI, 38.2-44.2) HRMs per 1000 beneficiaries in Medicare Advantage and to 56.9 (95% CI, 54.1-60.1) HRMs per 1000 beneficiaries in traditional Medicare. Across the study period, Medicare Advantage beneficiaries received 24.3 (95% CI, 20.2-28.3) fewer HRMs per 1000 beneficiaries per year compared with traditional Medicare beneficiaries. Female, American Indian or Alaska Native, and White populations were more likely to receive HRMs than other groups.
Results of this study showed that HRM rates were consistently lower among Medicare Advantage than traditional Medicare beneficiaries. Higher use of HRMs among female, American Indian or Alaska Native, and White populations is a concerning disparity that requires further attention.
限制老年人使用高风险药物(HRM)是国家的一项优先事项,目的是为医疗保险优势计划和传统按服务收费的医疗保险部分 D 计划的老年受益人提供高质量的护理。
评估传统医疗保险与医疗保险优势部分 D 计划的受益人之间 HRM 处方填写率的差异,并研究这些差异随时间的变化程度以及与较高 HRM 使用率相关的患者因素。
设计、设置和参与者:本队列研究使用了 2013 年至 2017 年医疗保险部分 D 数据中 20%的填药处方样本和 2018 年的 40%的样本。样本包括年龄在 66 岁或以上、参加医疗保险优势计划或传统医疗保险部分 D 计划的医疗保险受益人。数据分析于 2022 年 4 月 1 日至 2023 年 4 月 15 日进行。
主要结果是每 1000 名老年医疗保险受益人中规定的独特 HRM 数量。使用线性回归模型对主要结果进行建模,调整了患者特征和县特征,并包括医院转诊区域固定效应。
该样本包括 5595361 名独特的医疗保险优势受益人与 2013 年至 2018 年期间每年按比例匹配的 6578126 名独特的传统医疗保险受益人,共产生了 13704348 对受益年度的匹配对。传统医疗保险与医疗保险优势队列在年龄(平均[标准差]年龄,75.65[7.53]岁与 75.60[7.38]岁)、男性比例(8127261[59.3%]与 8137834[59.4%];标准化均差[SMD] = 0.002)和主要种族和民族(77.1%与 77.4%非西班牙裔白人;SMD = 0.05)方面相似。2013 年平均而言,医疗保险优势受益人的 1000 名受益人中有 135.1(95%置信区间,128.4-142.6)种独特的 HRM,而传统医疗保险中的 1000 名受益人中有 165.6(95%置信区间,158.1-172.3)种 HRM。2018 年,医疗保险优势受益人的 HRM 率已降至每 1000 名受益人 41.5(95%置信区间,38.2-44.2)种,而传统医疗保险中的 HRM 率已降至每 1000 名受益人 56.9(95%置信区间,54.1-60.1)种。在整个研究期间,医疗保险优势受益人的 HRM 每年比传统医疗保险受益人少 24.3(95%置信区间,20.2-28.3)种。女性、美国印第安人或阿拉斯加原住民和白人比其他群体更有可能接受 HRM。
本研究结果表明,医疗保险优势受益人的 HRM 率始终低于传统医疗保险受益人。女性、美国印第安人或阿拉斯加原住民和白人中较高的 HRM 使用是一个令人关注的差异,需要进一步关注。