Dubar Victoria, Pascreau Tiffany, Dupont Annabelle, Dubucquoi Sylvain, Dautigny Anne-Laure, Ghozlan Benoit, Zuber Benjamin, Mellot François, Vasse Marc, Susen Sophie, Poissy Julien, Gaudet Alexandre
CHU Lille, Pôle de Médecine Intensive-Réanimation, F-59000 Lille, France.
Biology Department, Hôpital Foch, F-92150 Suresnes, France.
Biomedicines. 2023 May 23;11(6):1504. doi: 10.3390/biomedicines11061504.
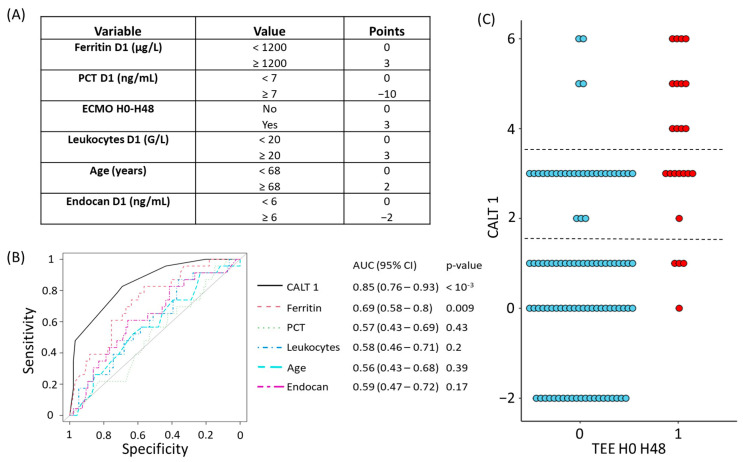
Severe COVID-19 infections are at high risk of causing thromboembolic events (TEEs). However, the usual exams may be unavailable or unreliable in predicting the risk of TEEs at admission or during hospitalization. We performed a retrospective analysis of two centers (n = 124 patients) including severe COVID-19 patients to determine the specific risk factors of TEEs in SARS-CoV-2 infection at admission and during stays at the intensive care unit (ICU). We used stepwise regression to create two composite scores in order to predict TEEs in the first 48 h (H0-H48) and during the first 15 days (D1-D15) in ICU. We then evaluated the performance of our scores in our cohort. During the period H0-H48, patients with a TEE diagnosis had higher D-Dimers and ferritin values at day 1 (D1) and day 3 (D3) and a greater drop in fibrinogen between D1 and D3 compared with patients without TEEs. Over the period D1-D15, patients with a diagnosis of a TEE showed a more marked drop in fibrinogen and had higher D-Dimers and lactate dehydrogenase (LDH) values at D1 and D3. Based on ROC analysis, the COVID-related acute lung and deep vein thrombosis (CALT) 1 score, calculated at D1, had a diagnostic performance for TEEs at H0-H48, estimated using an area under the curve (AUC) of 0.85 (CI95%: 0.76-0.93, < 10). The CALT 2 score, calculated at D3, predicted the occurrence of TEEs over the period D1-D15 with an estimated AUC of 0.85 (CI95%: 0.77-0.93, < 10). These two scores were used as the basis for the development of the CALT protocol, a tool to assist in the decision to use anticoagulation during severe SARS-CoV-2 infections. The CALT scores showed good performances in predicting the risk of TEEs in severe COVID-19 patients at admission and during ICU stays. They could, therefore, be used as a decision support protocol on whether or not to initiate therapeutic anticoagulation.
重症新型冠状病毒肺炎(COVID-19)感染极易引发血栓栓塞事件(TEE)。然而,常规检查在预测入院时或住院期间发生TEE的风险时可能无法进行或结果不可靠。我们对两个中心(共124例患者)进行了回顾性分析,这些患者均为重症COVID-19患者,目的是确定严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染患者入院时及在重症监护病房(ICU)住院期间发生TEE的具体危险因素。我们采用逐步回归分析创建了两个综合评分,以预测ICU中前48小时(H0-H48)和前15天(D1-D15)内发生TEE的情况。随后,我们评估了这些评分在我们研究队列中的表现。在H0-H48期间,与未发生TEE的患者相比,被诊断为TEE的患者在第1天(D1)和第3天(D3)的D-二聚体和铁蛋白值更高,且D1至D3期间纤维蛋白原下降幅度更大。在D1-D15期间,被诊断为TEE的患者纤维蛋白原下降更为明显,且在D1和D3时D-二聚体和乳酸脱氢酶(LDH)值更高。基于受试者工作特征(ROC)分析,在D1时计算得出的COVID相关急性肺和深静脉血栓形成(CALT)1评分对H0-H48期间TEE的诊断性能良好,使用曲线下面积(AUC)估计为0.85(95%置信区间:0.76-0.93,P<0.01)。在D3时计算得出的CALT 2评分预测了D1-D15期间TEE的发生情况,估计AUC为0.85(95%置信区间:0.77-0.93,P<0.01)。这两个评分被用作制定CALT方案的基础,该方案是一种在严重SARS-CoV-2感染期间辅助决定是否使用抗凝治疗的工具。CALT评分在预测重症COVID-19患者入院时及在ICU住院期间发生TEE的风险方面表现良好。因此,它们可作为是否启动治疗性抗凝的决策支持方案。