Infectious Diseases Division, Department of Diagnostics and Public Health, University of Verona, Verona, Italy.
Infectious Disease Unit, Mater Salutis Hospital - ULSS 9 Scaligera, Legnago, Italy.
Front Cell Infect Microbiol. 2023 Jun 12;13:1155320. doi: 10.3389/fcimb.2023.1155320. eCollection 2023.
Residency in LTCFs increases the likelihood of colonization with multidrug resistant Gram-negative bacteria (MDR-GNB). We assessed the prevalence and risk factors for enteric colonization by III-generation cephalosporins-resistant and carbapenem-resistant (CR) GNB in a large group of LTCFs in a high endemic setting. We also assessed the prevalence and risk factors for colonization.
A point prevalence survey with rectal screening (RS) was conducted in 27 LTCFs in north Italy. Epidemiological and clinical variables on the survey day, history of hospitalization and surgery within one year, and antibiotics within three months, were collected. The presence of III-generation cephalosporin resistant and CR GNB was assessed using a selective culture on chromogenic medium and PCR for carbapenemase detection. The presence of was assessed using ELISA for GDH and RT-PCR to identify toxigenic strains. Multi-variable analyses were performed using two-level logistic regression models.
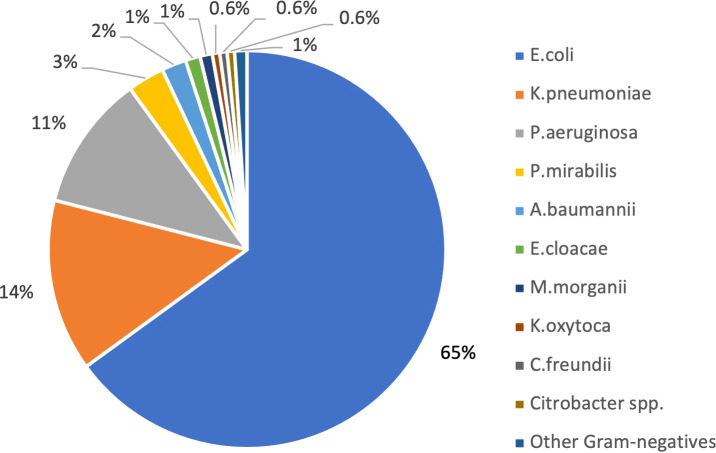
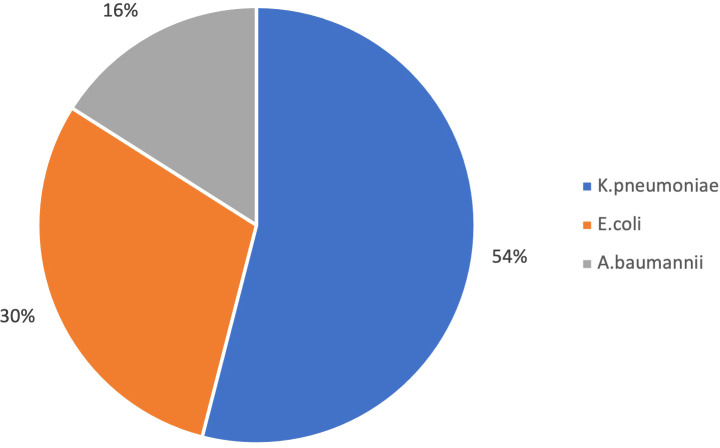
In the study period 1947 RSs were performed. The prevalence of colonization by at least one GNB resistant to III-generation cephalosporin was 51% ( 65%, 14% of isolates). The prevalence of colonization by CR GNB was 6%. 6% of all isolates (1150 strains) resulted in a carbapenem-resistant , and 3% in a carbapenem-resistant . KPC was the most frequent carbapenemase (73%) identified by PCR, followed by VIM (23%). The prevalence of colonization by was 11.7%. The presence of a medical device (OR 2.67) and previous antibiotic use (OR 1.48) were significantly associated with III-generation cephalosporin resistant GNB colonization. The presence of a medical device (OR 2.67) and previous hospitalization (OR 1.80) were significantly associated with CR GNB. The presence of a medical device (OR 2.30) was significantly associated with colonization. Main previously used antibiotic classes were fluoroquinolones (32% of previously treated subjects), III-generation cephalosporins (21%), and penicillins (19%).
Antimicrobial stewardship in LTCFs is a critical issue, being previous antibiotic treatment a risk factor for colonization by MDR-GNB. The prevalence of colonization by III-generation cephalosporin and CR GNB among LTCF residents also underlines the importance to adhere to hand hygiene indications, infection prevention and control measures, and environmental hygiene protocols, more achievable than rigorous contact precautions in this type of social setting.
在长期护理机构(LTCF)居住会增加对多重耐药革兰氏阴性菌(MDR-GNB)定植的可能性。我们评估了在高流行地区的一大群 LTCF 中,对第三代头孢菌素耐药和耐碳青霉烯(CR)的 GNB 的肠定植的患病率和危险因素。我们还评估了定植的患病率和危险因素。
在意大利北部的 27 家 LTCF 中进行了一项直肠筛查(RS)的点患病率调查。在调查当天收集流行病学和临床变量,一年内住院和手术史,以及三个月内抗生素使用情况。使用显色培养基进行选择性培养和 PCR 检测碳青霉烯酶来评估第三代头孢菌素耐药和 CR GNB 的存在。使用谷氨酸脱氢酶(GDH)ELISA 和 RT-PCR 检测产毒株来评估 定植的存在。使用两水平逻辑回归模型进行多变量分析。
在研究期间,共进行了 1947 次 RS。至少对一种三代头孢菌素耐药的 GNB 定植的患病率为 51%(65%,14%的分离株)。CR GNB 定植的患病率为 6%。所有分离株(1150 株)中有 6%为耐碳青霉烯的 ,3%为耐碳青霉烯的 。PCR 鉴定出的最常见的碳青霉烯酶是 KPC(73%),其次是 VIM(23%)。定植的患病率为 11.7%。存在医疗器械(OR 2.67)和先前使用抗生素(OR 1.48)与三代头孢菌素耐药 GNB 定植显著相关。存在医疗器械(OR 2.67)和先前住院(OR 1.80)与 CR GNB 定植显著相关。存在医疗器械(OR 2.30)与 定植显著相关。主要的先前使用的抗生素类别是氟喹诺酮类(32%的先前治疗患者)、三代头孢菌素(21%)和青霉素类(19%)。
在 LTCF 中进行抗菌药物管理是一个关键问题,因为先前的抗生素治疗是 MDR-GNB 定植的危险因素。LTCF 居民中第三代头孢菌素和 CR GNB 的定植率也强调了遵守手卫生指征、感染预防和控制措施以及环境卫生方案的重要性,这些方案在这种社会环境中比严格的接触预防更容易实现。