Center for Robotic Simulation and Education, Catherine and Joseph Aresty Department of Urology, USC Institute of Urology, University of Southern California, Los Angeles.
Department of Urology, Weill Cornell Medicine, New York, New York.
JAMA Netw Open. 2023 Jun 1;6(6):e2320702. doi: 10.1001/jamanetworkopen.2023.20702.
Live feedback in the operating room is essential in surgical training. Despite the role this feedback plays in developing surgical skills, an accepted methodology to characterize the salient features of feedback has not been defined.
To quantify the intraoperative feedback provided to trainees during live surgical cases and propose a standardized deconstruction for feedback.
DESIGN, SETTING, AND PARTICIPANTS: In this qualitative study using a mixed methods analysis, surgeons at a single academic tertiary care hospital were audio and video recorded in the operating room from April to October 2022. Urological residents, fellows, and faculty attending surgeons involved in robotic teaching cases during which trainees had active control of the robotic console for at least some portion of a surgery were eligible to voluntarily participate. Feedback was time stamped and transcribed verbatim. An iterative coding process was performed using recordings and transcript data until recurring themes emerged.
Feedback in audiovisual recorded surgery.
The primary outcomes were the reliability and generalizability of a feedback classification system in characterizing surgical feedback. Secondary outcomes included assessing the utility of our system.
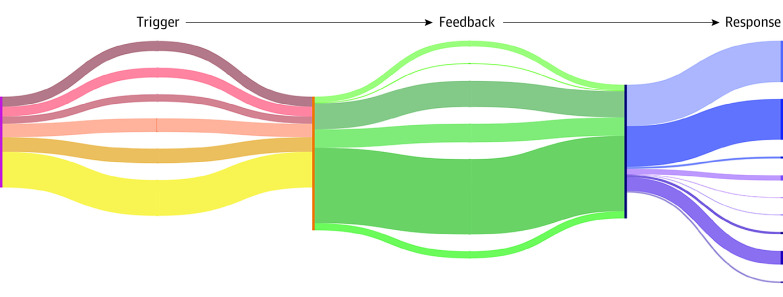
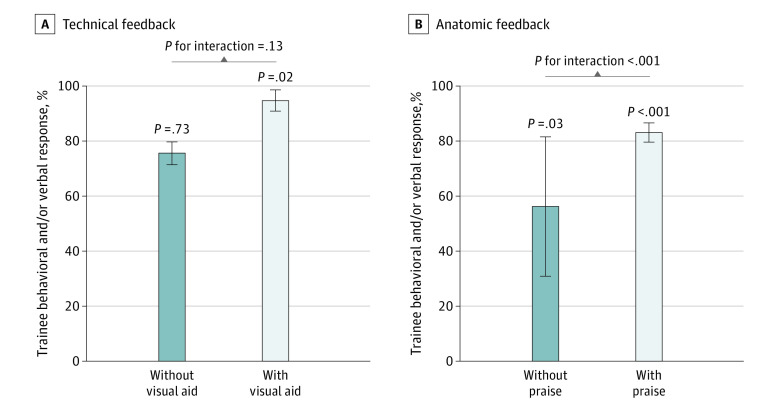
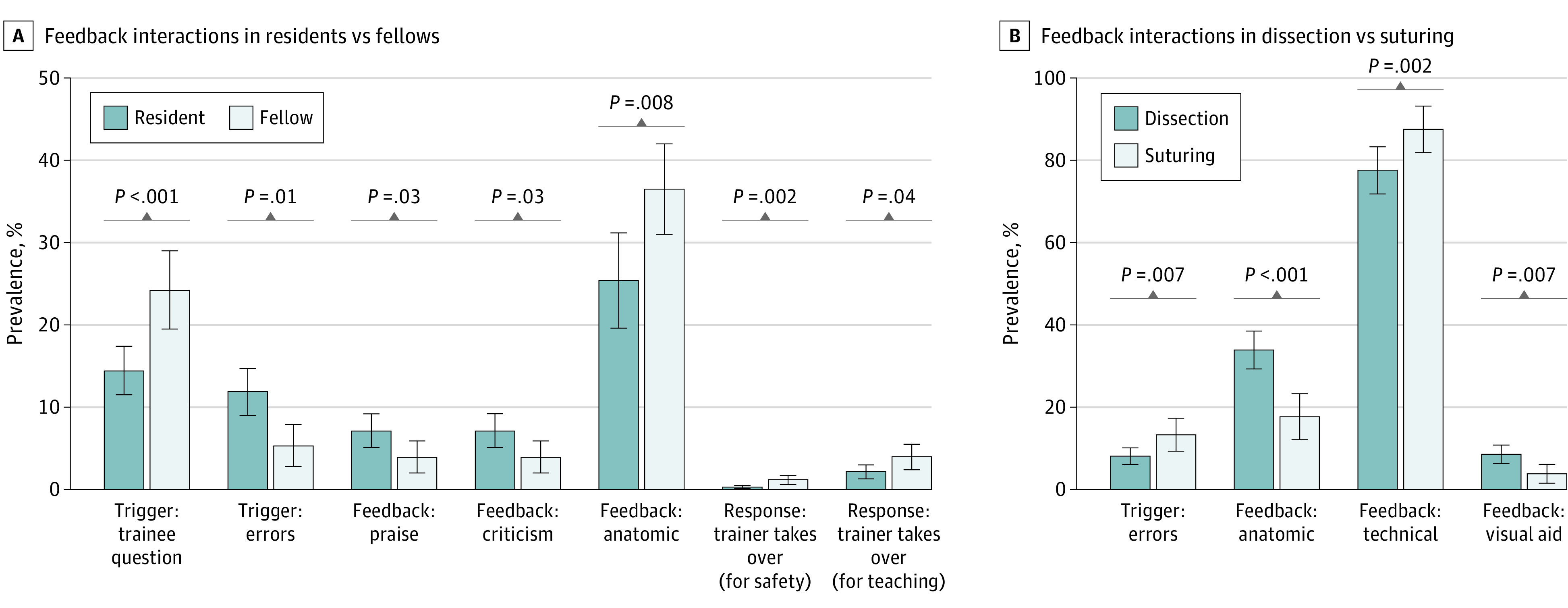
In 29 surgical procedures that were recorded and analyzed, 4 attending surgeons, 6 minimally invasive surgery fellows, and 5 residents (postgraduate years, 3-5) were involved. For the reliability of the system, 3 trained raters achieved moderate to substantial interrater reliability in coding cases using 5 types of triggers, 6 types of feedback, and 9 types of responses (prevalence-adjusted and bias-adjusted κ range: a 0.56 [95% CI, 0.45-0.68] minimum for triggers to a 0.99 [95% CI, 0.97-1.00] maximum for feedback and responses). For the generalizability of the system, 6 types of surgical procedures and 3711 instances of feedback were analyzed and coded with types of triggers, feedback, and responses. Significant differences in triggers, feedback, and responses reflected surgeon experience level and surgical task being performed. For example, as a response, attending surgeons took over for safety concerns more often for fellows than residents (prevalence rate ratio [RR], 3.97 [95% CI, 3.12-4.82]; P = .002), and suturing involved more errors that triggered feedback than dissection (RR, 1.65 [95% CI, 1.03-3.33]; P = .007). For the utility of the system, different combinations of trainer feedback had associations with rates of different trainee responses. For example, technical feedback with a visual component was associated with an increased rate of trainee behavioral change or verbal acknowledgment responses (RR, 1.11 [95% CI, 1.03-1.20]; P = .02).
These findings suggest that identifying different types of triggers, feedback, and responses may be a feasible and reliable method for classifying surgical feedback across several robotic procedures. Outcomes suggest that a system that can be generalized across surgical specialties and for trainees of different experience levels may help galvanize novel surgical education strategies.
在外科培训中,手术室中的实时反馈至关重要。尽管这种反馈在培养手术技能方面发挥了作用,但尚未定义一种被接受的方法来描述反馈的显著特征。
量化在活体手术中向学员提供的术中反馈,并提出一种标准化的反馈解构方法。
设计、设置和参与者:在这项使用混合方法分析的定性研究中,在 2022 年 4 月至 10 月期间,在一家学术性三级护理医院的手术室中对外科医生进行了音频和视频记录。有资格自愿参加的是参与机器人教学病例的泌尿科住院医师、研究员和主治外科医生,这些病例中,学员在手术的至少一部分时间里主动控制机器人控制台。反馈被标记时间并逐字转录。使用录音和转录数据进行迭代编码过程,直到出现重复主题。
视听记录手术中的反馈。
主要结果是反馈分类系统在描述手术反馈方面的可靠性和通用性。次要结果包括评估我们系统的实用性。
在记录和分析的 29 个手术过程中,涉及 4 名主治外科医生、6 名微创外科研究员和 5 名住院医师(研究生年级 3-5 年级)。对于系统的可靠性,3 名经过培训的评估者在使用 5 种触发因素、6 种反馈和 9 种反应(患病率调整和偏差调整κ范围:从触发因素的 0.56 [95% CI,0.45-0.68]到反馈和反应的 0.99 [95% CI,0.97-1.00]的最低值到最大值)对病例进行编码时达到了中度至高度的评估者间可靠性。对于系统的通用性,对 6 种手术程序和 3711 次反馈进行了分析和编码,包括触发因素、反馈和反应类型。触发因素、反馈和反应的显著差异反映了外科医生的经验水平和正在进行的手术任务。例如,作为一种反应,主治外科医生因安全问题更频繁地为研究员而非住院医师接管(患病率比[RR],3.97 [95% CI,3.12-4.82];P = .002),缝合比解剖更容易出现触发反馈的错误(RR,1.65 [95% CI,1.03-3.33];P = .007)。对于系统的实用性,不同的培训师反馈组合与不同学员反应的发生率有关。例如,具有视觉成分的技术反馈与学员行为改变或口头确认反应的增加率相关(RR,1.11 [95% CI,1.03-1.20];P = .02)。
这些发现表明,识别不同类型的触发因素、反馈和反应可能是一种可行且可靠的方法,可以对几种机器人手术中的反馈进行分类。研究结果表明,一种可以在外科专业和不同经验水平的学员中通用的系统,可能有助于激发新的外科教育策略。