Facility of Medicine and Health Sciences, University of Auckland, Auckland, New Zealand.
Department of Medicine, University of Otago, Christchurch, New Zealand.
Drugs Aging. 2023 Sep;40(9):847-855. doi: 10.1007/s40266-023-01044-2. Epub 2023 Jun 29.
Medication adherence improves morbidity and mortality-related outcomes in heart failure, and knowledge of patterns of medication adherence supports patient and clinician decision-making. Routinely collected national data facilitate the exploration of medication adherence and associated factors in older adults with heart failure, including the association between ethnicity and adherence. There are known inequities in access to medicines between Māori (Indigenous People of Aotearoa New Zealand) and non-Māori, yet ethnic variation in medicines adherence in community-dwelling older adults with heart failure has not been explored.
Here we identify medication adherence rates for community-dwelling older adults diagnosed with heart failure and differences in adherence rates between Māori and non-Māori.
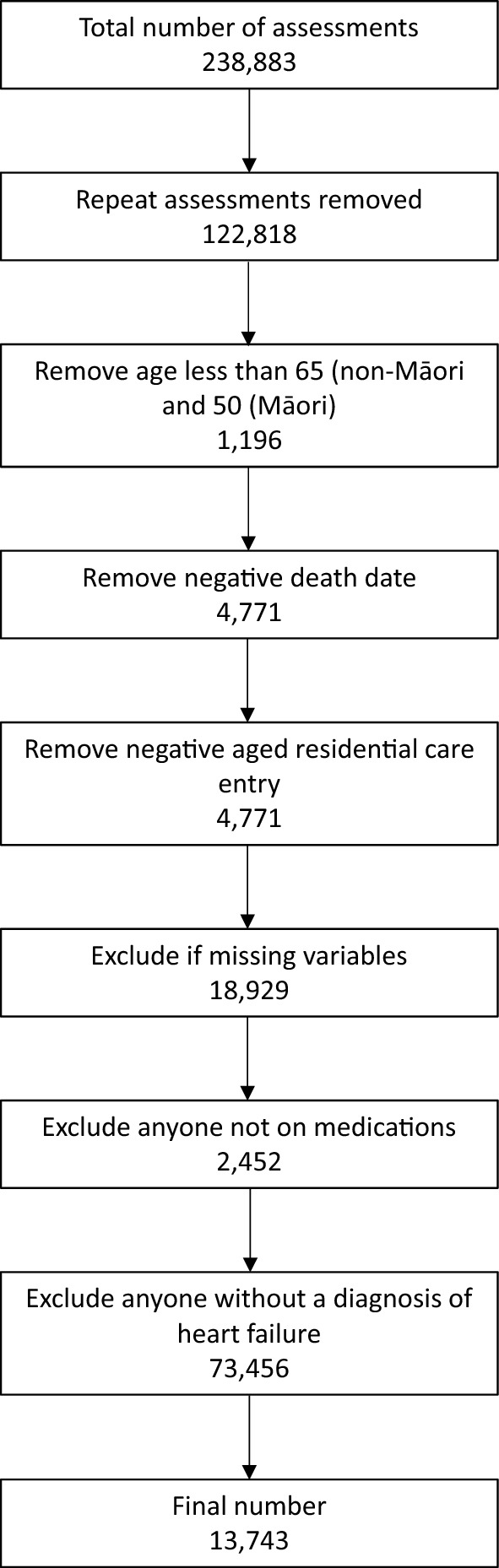
Cross-sectional analysis of interRAI (comprehensive standardised assessment) data in a continuously recruited national cohort from 2012 to 2019.
Overall, 13,743 assessments (Māori N = 1526) for older community-dwelling adults with heart failure diagnoses were included. The mean age of participants was 74.5 years [standard deviation (SD) 9.1 years] for Māori and 82.3 years (SD 7.8 years) non-Māori. In the Māori cohort, 21.8% did not adhere fully to their medication regimen, whereas in the non-Māori cohort, this figure was 12.8%. After adjusting for confounders, the Māori cohort were more likely to be medication non-adherent than non-Māori [prevalence ratio 1.53, 95% confidence interval (CI) 1.36-1.73].
There was a significant disparity between Māori and non-Māori concerning medication adherence. Given the international use of the interRAI-HC assessment tool, these results have significant transferability to other countries and allow the identification of underserved ethnic groups for which culturally appropriate interventions can be targeted.
药物依从性可改善心力衰竭患者的发病率和死亡率相关结局,而对药物依从性模式的了解则有助于患者和临床医生做出决策。常规收集的国家数据有助于探索心力衰竭老年患者的药物依从性及其相关因素,包括族裔与依从性之间的关系。毛利人(新西兰原住民)和非毛利人在获得药物方面存在明显的不平等,但尚未探讨社区居住的心力衰竭老年患者中药物依从性的族裔差异。
本研究旨在确定社区居住的心力衰竭老年患者的药物依从性率,并比较毛利人和非毛利人之间的药物依从性率差异。
对 2012 年至 2019 年连续招募的全国队列中使用 interRAI(综合标准化评估)数据进行横断面分析。
共有 13743 例(毛利人 N=1526)社区居住的心力衰竭老年患者的评估结果纳入本研究。参与者的平均年龄为 74.5 岁(标准差 [SD] 9.1 岁),毛利人组为 21.8%未完全遵医嘱服药,而非毛利人组为 12.8%。调整混杂因素后,与非毛利人相比,毛利人更有可能不遵医嘱服药[比值比 1.53,95%置信区间(CI)1.36-1.73]。
毛利人和非毛利人之间在药物依从性方面存在显著差异。鉴于 interRAI-HC 评估工具在国际上的应用,这些结果具有重要的可转移性,可适用于其他国家,并确定需要针对性开展文化适宜性干预的服务不足的族裔群体。